

Introduction
According to the WHO classification (4th edition, 2017), odontogenic cysts of inflammatory origin are classified into radicular cysts including residual cysts or inflammatory collateral cysts. The latter is also subclassified into paradental cysts and mandibular buccal bifurcation cysts.1
In a retrospective study conducted to determine the range of diagnosed odontogenic cysts with age, researchers analysed 55,446 specimens to determine the prevalence of diagnosed odontogenic cysts. Out of the total specimens, 7,121 (12.8%) were identified as having odontogenic cysts.2 The predominant diagnostic category was the radicular cyst, constituting 52.3% of all odontogenic cysts (3,724 cases). Adults exhibited a higher prevalence of radicular cysts (3,359 cases), comprising 52.6% of the overall cases, compared to paediatric patients (241 cases) at 43.6%. Residual cysts made up 8% of the total cases (573), with 555 cases found in adults, indicating a higher occurrence in adults than in paediatric patients. A total of 402 paradental cysts were observed, with a twofold higher incidence in adults (5.9%) compared to children (2.7%).2 Buccal bifurcation cysts have a higher prevalence among paediatric populations, primarily manifesting in the buccal region with the eruption of the first molar.3
Radicular cysts are chronic inflammatory lesions developed pathologically by inflammation to proliferate the epithelial rests of Malassez, and they are associated with non-vital teeth. Radiographically, the cyst is characterised by an unilocular, well-defined corticated periapical radiolucency associated with the apex of non-vital teeth.4,5
Histologically, the central lumen is supported by a fibrous connective tissue wall and lined with non-keratinised stratified squamous epithelium. Inflammatory cell infiltrates ranging from mild to heavy are frequently observed, with fluid or cellular debris filling the lumen.4
The term ‘inflammatory collateral cyst’ refers to cysts that develop on the buccal surface of the roots of partially or recently erupted teeth due to peri-coronal tissue inflammation.1 Paradental cysts are associated with partially erupted mandibular wisdom teeth with a history of pericoronitis, whereas mandibular buccal bifurcation cysts develop on the lower first or second molars.1
This report presents a detailed analysis of a very uncommon occurrence of an inflammatory odontogenic cyst that probably originated from an enamel pearl located in the furcation of the upper left first molar (UL6) in a young patient.
Case report
A 14-year-old girl was referred to the Orthodontic Department at Royal London Dental Hospital (RLDH) with crowding in her permanent canines, which required orthodontic treatment. The patient reported to the Department of Oral and Maxillofacial Surgery at RLDH with a chief complaint of a large radiolucent lesion attached to the UL6. On extra-oral examination, nothing abnormal was discovered and the intra-oral examination of UL6 revealed that the tooth was sound with no evidence of pathology, but demonstrated non-vitality with application of Endo Frost Spray. Pre-operative clinical photographs are shown in Figure 1.

Radiographic examination
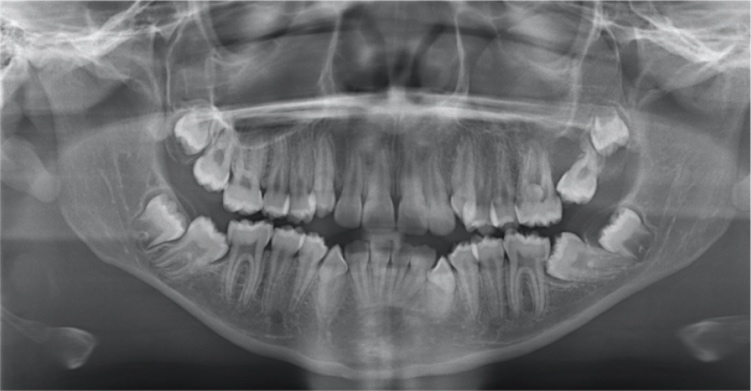
An orthopantomogram (OPG) (Figure 2) showed an enamel pearl measuring up to 5.7mm by 5mm lying within the furcation of UL6 with a large, well-defined corticated radiolucency lesion measuring up to 45mm by 43mm attached to the apices of the UL6. The radiolucency overlapped the left maxillary sinus and extended superiorly. The upper left second molar (UL7) was mesioangular, abutted to the distal aspect of the UL6, and was severely displaced due to the cyst development.

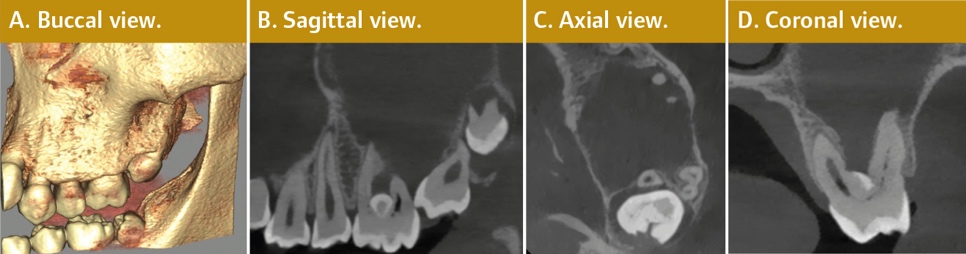
Cone-beam computed tomography (CBCT) showed a large, well-defined corticated radiolucency extending beyond the superior edge of this volume (Figure 3B). The radiolucency filled the left maxillary sinus and displaced the sinus floor superiorly. The radiolucency was centred on UL6, with an enamel pearl lying within its furcation, as shown in Figure 3D. There was a dehiscence of the alveolar crest between the crowns of UL6 and UL7 associated with slight buccopalatal expansion, as shown in Figure 3C. The UL7 was mesioangular, and abutted the distal aspect of UL6 at the approximate level of the cemento-enamel junction (CEJ), as shown in Figures 3A and 3B.

Differential diagnosis
The clinical and radiographic findings were suggestive of a differential diagnosis as follows: (i) radicular cyst or large periapical granuloma; (ii) collateral inflammatory cyst; or, (iii) odontogenic keratocyst. The first stage of the treatment plan was surgical extraction of UL6 with cyst enucleation and histopathological examination, to confirm the diagnosis and monitor the eruption of UL7 and the bone levels around it. Ultimately, after reviewing the benefits and risks of these procedures, the patient and her mother consented to have all surgical procedures performed in a single appointment under general anaesthesia.
Management and intervention
One of the challenges was preserving the UL7. During the procedure, the UL6 extraction was difficult due to the existence of the enamel pearl engaged in the buccal bone, which necessitated surgical extraction of UL6 to preserve UL7. The surgery started with the surgical extraction of UL6 with a three-sided flap and the UL6 was sectioned into many pieces so that it could be extracted without applying additional force on the adjacent UL7, (Figure 4). The cyst was enucleated with special care for the maxillary sinus. Subsequently, UL6 and the cyst pieces were sent for histopathology examination to confirm the diagnosis. Despite the presence of a substantial bone defect at the surgical site, UL7 was eventually saved in its position.

Macroscopic and microscopic findings
Hematoxylin and eosin (H&E) staining demonstrated multiple, brown-coloured soft tissue pieces. Microscopic examination showed fibrous and granulation-walled cyst fragments lined in part by non-keratinised stratified squamous epithelium with a dense, patchy, mixed inflammatory infiltrate. The histological examination confirmed that the lesion was an inflammatory odontogenic cyst with non-specific features.
Discussion
The process of definitively diagnosing oral lesions may be challenging due to the presence of some lesions that closely resemble others. Therefore, the correlation between clinical and radiographic findings and microscopic features is vital to confirm the diagnosis and formulate a treatment plan for such lesions.
The typical pathogenesis of inflammatory periapical lesions is initiated by caries or dental trauma, which results in pulp necrosis and bacterial invasion of the periapical region. This may progress into an acute or chronic dentoalveolar abscess or the formation of a periapical granuloma or radicular cyst.6 Paradental cysts are often seen in cases when mandibular wisdom teeth have only partially erupted and had an underlying diagnosis of pericoronitis. In these instances, the inflammatory response triggers the proliferation of the reduced enamel epithelium or the sulcular or junctional epithelium, leading to the formation of the cyst lining.
In the literature review, a number of terminologies are used to describe the same lesion, including paradental cyst, infected buccal cyst, and buccal bifurcation cyst. From a histological perspective, these entities exhibit histopathological characteristics similar to radicular cysts, but they are identified as pericoronal in terms of their morphological and radiographic features.7
Extremely rarely, cervical enamel extension, also known as enamel pearl, can develop along the surface of dental roots, particularly molars, and may be one of the rare causes of inflammatory cysts.8,9 Enamel projection into the furcation of molars is one of the uncommon causes of this type of cyst, but it is of note that the source of the epithelium in such cases could be derived from the apically directed epithelial attachment and post-eruptive expansion of the reduced enamel epithelium during the tooth eruption.5 Therefore, this must be associated with a source of infection to proliferate the lining epithelium, which contributes to the formation of the cyst. Scientific evidence has shown that bacterial plaque is the main component responsible for the development and advancement of periodontal disease. This is particularly true when combined with anatomical factors like ectopic enamel, which contribute to advanced localised periodontal destruction,10 and are associated with a predisposition to attachment loss.11
The enamel pearl can be considered a risk factor that contributes to the development of inflammatory cysts rather than being the direct cause. This is because the presence of an enamel pearl increases the likelihood of periodontal disease progressing at the furcation of teeth with multiple roots within the course of the epithelium, which derives from the apically directed epithelial attachment and post-eruptive expansion of the reduced enamel epithelium.
There is a lack of literature on this issue; no high-quality study has discussed the risk of inflammatory cyst development for such reasons in as our case, and no case report has described a cyst that develops from enamel pearls. Moreover, there is confusion regarding the terminologies for collateral inflammatory cysts and what has been discovered is only related to paradental cysts raised in partially erupted third molars or buccal bifurcation cysts raised by periodontal diseases.
In future dental examinations, it may be reasonable to consider the presence of enamel pearls as a risk factor for the development of inflammatory cysts. Furthermore, it may be concluded from the present case report that regular monitoring may be necessary for such instances to detect any early cystic-like changes and prevent the need for invasive jaw surgery.
Conclusion
Inflammatory odontogenic cysts are less prevalent in paediatric populations compared to adults. They are often present with clinical indicators including carious dentition, retained roots, failed root canal therapy, or a previous history of dental trauma resulting in necrotic pulp infiltration into the periapical area. Nevertheless, the occurrence of cysts in sound teeth is rare. The identification of enamel pearls located at the furcation of multi-rooted teeth may indicate a potential aetiological factor in the formation of inflammatory cysts, as discussed in the context of oral and maxillofacial pathology, which is considered to be rather infrequent. It is important to note that no case report like the present case has been identified, and the underlying disease process lacks a definitive aetiology for discussion.
Acknowledgement
Our greatest appreciation goes to our colleagues, who provided unconditional support during the preparation of this report. We would like to acknowledge the Orthodontic Department at RLDH and staff nurses for their assistance.