
Introduction
Temporomandibular disorder (TMD) represents a group of disorders related to the impairment of the temporomandibular joints (TMJ) and the associated neuromuscular system, which commonly present with features such as pain in the orofacial region, headache, joint sounds (click or crepitus), and disturbances in jaw movements.1 It is prevalent in society, affecting up to 50% of the general population, and is now considered to be the third most common chronic pain problem after headache and backache.2 Females are twice as likely to be affected as males, and usually reach a peak incidence in the second and third decades of life.3 The psychological and physical ailments caused by TMD are debilitating and can result in a lower quality of life in patients.3 The multifactorial aetiology of TMD is complex and remains unclear. Various predisposing, initiating, or perpetuating factors that work alone or in combination have been proposed to contribute to TMD. These include mechanical displacement, trauma, and biomedical, muscular, neuromuscular, and psychophysiological factors.4
TMD can be divided into four categories: myogenous TMD; arthrogenous TMD; chronic mandibular hypomobility; and, growth disorders.5 Arthrogenous TMD can be further subdivided into three major categories: derangement of the condyle-disc complex; structural incompatibility with articular surfaces; and, inflammatory disorders of the joint.5 The correct diagnosis of TMD is crucial as it allows for an effective treatment regime to be implemented. The current gold standard for research is the Research Diagnostic Criteria for TMD (RDC/TMD), which utilises both a physical and psychological approach to diagnosing and classifying patients with TMD.1 The physical component groups TMD into three groups: muscular disorders; temporomandibular disc displacement; and, joint disorders. This includes: signs and symptoms of tenderness of masticatory muscle on palpation; persistent orofacial pain; limitations in jaw movements; and, joint sounds. The psychological component measures quality of life, involving psychometric tests for disability, depression, and somatisation.1 A simpler method for diagnosis is the use of the Clinical Examination Protocol (CEP-TMD). Although this does not provide a psychosocial profile of the patient, it is a feasible method as it correlates well with the RDC/TMD.6
Myogenous TMD is categorised into myofascial pain with or without limited mouth opening.6 Myofascial pain includes features of three or more tender muscle sites on palpation and persistent pain that presents on the ipsilateral side as the palpation pain.1 Typical sites of pain in myogenous TMD include jaw pain, facial pain (temporal, frontal, and occipital), neck pain and earaches. The pain is often described as a constant dull ache, radiating along the head and neck region, which usually interferes with eating and sleeping.4 Furthermore, these patients usually present with deep and localised areas of tenderness (trigger points) that are located within taut bands of skeletal muscle. Digital palpation of these areas causes localised tenderness or referred tenderness towards the zone of reference.7 Limitation of mouth opening is noted as being less than 40mm with a passive stretch of 5mm or more. This may be attributed to inflammation of the muscle fascicles, which increases the viscoelastic tone and thus stiffness of the muscle, guarding response to pain.8
According to the American Association of Dental Research, the current first line of treatment for patients with TMD should be the use of conservative, reversible, and evidence-based options as opposed to invasive surgical treatments.9 These include: behavioural therapy (elimination of parafunctional habits, relaxation therapy, hypnosis); physical therapy (jaw exercises, postural training, thermal packs, manual therapy, acupuncture);use of occlusal appliances; and, pharmacotherapy (non-steroidal anti-inflammatory drugs (NSAIDs), muscle relaxants, tricyclic antidepressants), all of which are reported to be effective in alleviating TMD pain.10 However, due to uncertainties regarding the underlying patho-aetiology of TMD, a multimodal approach of conservative treatments is recommended.11 There is an increasing trend towards the use of botulinum toxin type-A (BTX-A) as an adjuvant treatment for TMD.12 In addition, recent studies have shown promising results to support the use of BTX-A in the management of TMD, establishing it as a safe, reversible, and conservative treatment option.8,13–17 As the main objective for TMD management is alleviating the signs and symptoms of the disorder, should there be a shift in the current treatment paradigm to include BTX-A as a first line of treatment? This retrospective study aims to investigate the effectiveness of BTX-A for the management of myogenous TMD and its potential to be included as a first line of treatment.
Materials and methods
A retrospective search was carried out through the Oral and Maxillofacial Department’s logbook in University Hospital Galway from January 1, 2016, to December 31, 2020. Patients who received BTX-A for the management of myogenous TMD were identified and their hospital electronic records were accessed. The patients’ age, gender, baseline and post-operative self-perceived pain scores, sites of injection, and adverse effects were recorded. From these records, pain improvement outcome was tabulated and recorded.
Results
From January 1, 2016, to December 31, 2020, 60 patients were diagnosed with myogenous TMD according to the CEP-TMD and were asked to evaluate the level of pain based on a numeric rating scale (1 being the least pain and 10 being the worst pain). These patients were managed conservatively with soft diet, NSAIDs, warm massages, soft occlusal appliances, and intramuscular injections of BTX-A at sites dependent on each patient’s complaint. Some 45 and 15 units of BTX-A (Dysport, Ipsen Biopharm, Wrexham, United Kingdom) were administered to masseter and temporalis muscles, respectively, at three different points. Review appointments were scheduled at four months postoperatively and patients were asked to evaluate the level of pain using the same numeric rating scale.
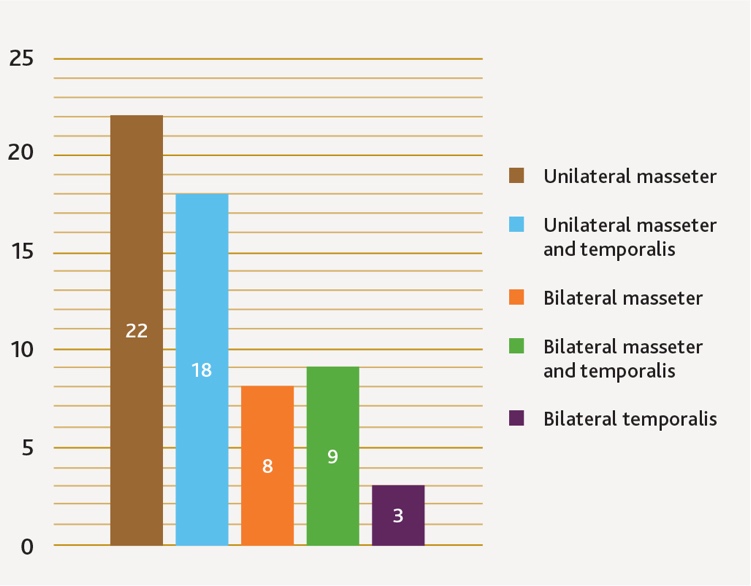
Of the 60 patients, there were 48 females (80%) and 12 males (20%). The mean age was 42 years for females (range 18 to 72) and 43 years for males (range 23 to 78). Twenty-two patients (37%) were diagnosed with unilateral masseter as the target muscle, 18 patients (30%) with unilateral masseter and temporal muscles, nine patients (15%) with bilateral masseter and temporal muscles, eight patients (13%) with bilateral masseter muscles and three patients (5%) with bilateral temporal muscles (Figure 1).

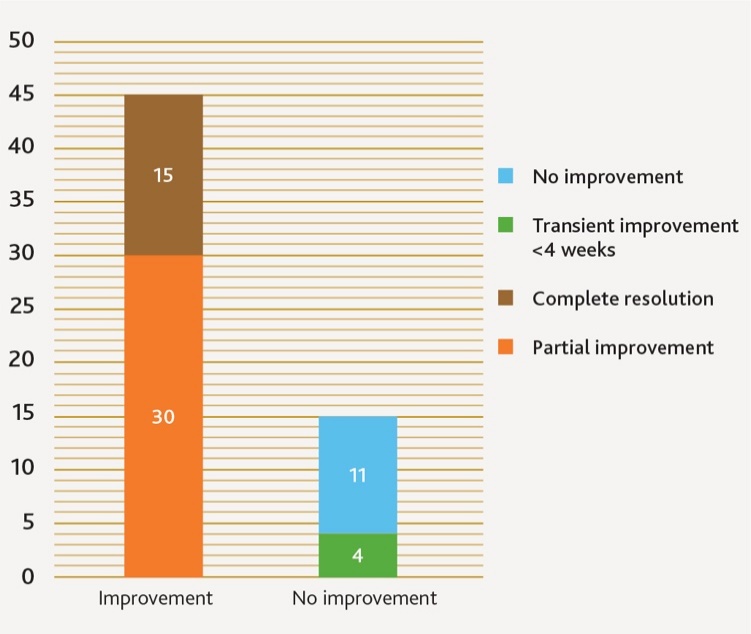
The mean baseline level of pain was scored at 8 and the mean postoperative level of pain at four months was scored at 4, giving a mean of 50% improvement in the level of self-perceived pain. Forty-five patients (75%) reported improvement in pain levels, of whom 10 (17%) reported complete resolution of pain. Fifteen patients (25%) reported no improvement in pain levels, of whom four (7%) reported transient improvement lasting four weeks (Figure 2). Thirty-five of the 45 patients also reported a reduction in NSAID intake, while the remaining 10 reported a stoppage of NSAID intake.

Discussion
This study included a greater proportion of female patients (80%) as compared to males (20%), which is similarly reflected in epidemiological studies.3 Despite discussion of various factors such as hormonal, psychosocial, behavioural, and biomedical, no conclusions have yet to been drawn to explain the difference.4
Botulinum toxin
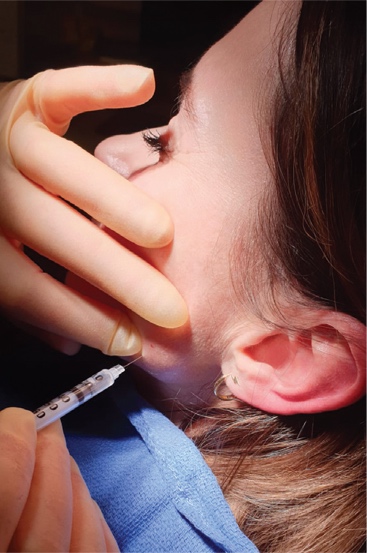
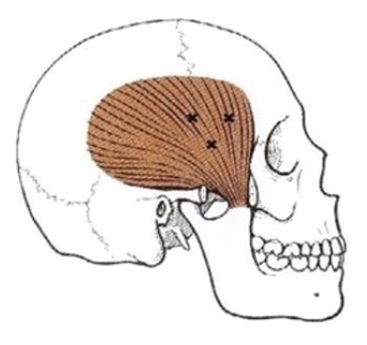
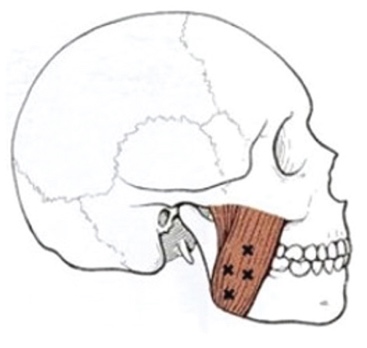
Botulinum toxin is a 150-kilodalton potent exotoxin produced by the gram-positive anaerobic bacterium Clostridium botulinum.18 Of the seven different subtypes (A to G), BTX-A acts as a pre-synaptic neurotoxin, causing dose-dependent weakness or paralysis in skeletal muscles by cleaving docking proteins on membranes, which leads to the inhibition of acetylcholine release at motor nerve endings.19 Although alpha motor neuron function is primarily affected, BTX-A may also affect gamma motor neurons, which lowers the resting tone of muscles.19 In addition, BTX-A has been shown to inhibit the release of inflammatory neuropeptides from sensory neurons such as substance P and calcitonin gene-related peptides, resulting in a reduction of inflammatory pain and a rise in pain threshold.20 Thus, these synergistic effects of BTX-A make it applicable for the management of myogenous TMD. As directed by manufacturers, 100U of freeze-dried BTX-A is reconstituted with 1ml of room temperature sterile saline and is delivered to the muscles with the use of a 1ml 31-gauge insulin needle (Figures 3 and 4). Due to the difficulty in locating the pterygoid muscles, the temporal (Figure 5) and masseter muscles (Figure 6) are typically the target muscles for the injection.13,14,17,21 Despite numerous studies, there is still a lack of consensus on the optimal dosage, varying from 50U unilaterally to 300U bilaterally.14,22 More research should be carried out to determine the optimal dosage and target sites.12
.jpeg)
.jpeg)


Efficacy of BTX-A treatment
Forty-five patients (75%) reported improvement in pain levels with the mean improvement of 50%. This shows promising results from the inclusion of BTX-A as a first line of conservative management of myogenous TMD, and this is similarly reflected in several clinical trials. A Canadian study of 46 subjects diagnosed with TMD reported a reduction in subjective pain in 87% of the subjects after intramuscular injection of BTX-A.8 In addition, a German study of 90 patients who had not responded initially to conservative treatments reported improvement in painful symptoms for 90% of the study group.16 Similarly, another study reported reduction in pain for both study group (BTX-A) and a control group (saline) that was crossed over to the BTX-A group later in the study.15 Patients suffering from TMD due to bruxism have also been reported to benefit from BTX-A in terms of improvement in range of mandibular movements.13,17 Furthermore, BTX-A has been shown to be as effective as conservative treatments such as fascial manipulation.14 However, limitations in these studies include heterogeneity of study designs, short follow-up periods, and small sample sizes. In addition, results from two other studies have reported no relevant clinical effects of BTX-A for the management of TMD.21,22
Limitations of BTX-A treatment
Four patients reported transient relief in pain symptoms lasting four weeks. This may be due to the reversible effects of BTX-A, attributed to the regrowth of neurons that occurs after two to four months.19 This questions the long-term benefits and may indicate the need for repeated injections. Furthermore, due to its immunogenic properties, repeated exposure to BTX-A protein complex may lead to the stimulation of antibody production, causing interference to its activity.23 As a result, repeated treatment can reduce its effectiveness and add to the burden of cumulative costs. However, relief of symptoms beyond the expected pharmacokinetic duration of BTX-A has been reported, suggesting a possible neuromodulating effect of the drug at the level of the central nervous system.24 Therefore, despite promising results, recent systematic reviews have concluded that there is a need for more high-quality research with larger sample sizes, minimal bias, and longer follow-up periods.12
Adverse effects of BTX-A
The use of BTX-A is associated with various adverse effects, albeit minor and transient. One study reported adverse effects during the treatment of headache disorders, such as blepharoptosis, brow ptosis, diplopia, and muscle weakness at injection sites.25 Other adverse effects experienced by patients include flu-like symptoms, dry mouth, dysphagia, localised pain and focal muscle weakness, which may result in an asymmetrical smile.13,21,22 However, no major or long-term adverse effects have been reported.12 This has been reflected similarly in this study where no adverse effects were reported. Thus, together with the reversible nature of BTX-A, this renders the use of BTX-A as minimally invasive.
Efficacy of current conservative treatments
Conservative treatments such as behavioural therapy, physical therapy, use of occlusal appliances, and pharmacotherapy are currently regarded as the first line of treatment for the management of TMD, with success rates around 70%.9 However, there is a lack of evidence to support the effectiveness of oral splints in relieving pain in TMD.26 Furthermore, there is still great uncertainty about the effectiveness of manual therapy for TMD.27 Despite having proven effectiveness in reducing pain in TMD, long-term pharmacological treatments such as NSAIDs may be harmful due to adverse effects such as gastrointestinal effects and worsening renal function.28 Therefore, this demonstrates some limitations in the current approach to the management of TMD.
Conclusion
Currently, BTX-A is only regarded as an adjuvant treatment when standard conservative treatments have failed.29 However, with its reversible nature and high safety margins, BTX-A should be considered as a minimally invasive treatment. As a multimodal approach is recommended due to the complexity of the patho-aetiology of TMD, the combination of BTX-A with other traditional conservative treatments could potentially improve outcomes. In addition, as some studies have demonstrated, effective results from BTX-A in participants where conservative treatments have failed,8,17,18,30 means the inclusion of BTX-A in the first line of treatment could result in more favourable outcomes. BTX-A has shown great potential and may shift the current treatment paradigm to include it as a first line of treatment for myogenous TMD. However, there remains the need for more high-quality research with larger sample sizes, minimal bias, and longer follow-up periods.