
Introduction
Population ageing in Northern Ireland (NI) is accelerating, with individuals aged ≥65 years currently representing approximately one-sixth of the population, and this proportion projected to increase substantially over the next 25 years.1 These changing age demographics will have significant implications for the provision of oral health, as a proportion of the ageing population will be dependent on others for care provision.
The oral health needs of the care-dependent population have changed dramatically over the last few decades.2,3 Dry mouth, chewing problems and swallowing difficulties are now commonly seen in vulnerable older people.4 Care for this group in the past encompassed more straightforward plans, to include mechanical plaque removal and cleaning of complete dentures. Now the retention of natural teeth in older people is becoming more common and their care needs are becoming more complex.5 While the retention of teeth represents an element of public health success, it also increases the complexity of treatment required and complicates the logistics of providing care for care-dependent individuals.
National surveillance through the United Kingdom Adult Dental Health Survey (ADHS) provides valuable longitudinal oral health data on a population level; however, care home residents are excluded from the screening programme. Difficulties are reported in assessing the oral health status of this cohort due to challenging behavioural issues, varying cognitive status, and decline in psychological state. When entering the care home system, access to dental services can become difficult due to mobility constraints and pre-existing comorbidities.6 The collection of patient data for epidemiological studies in this cohort is challenging, and data are often inaccurate. Consequently, the oral health status of institutionalised older adults remains poorly characterised. International studies suggest higher levels of untreated disease, tooth loss, and unmet need in nursing home residents compared with their community-living peers.7
In NI, the majority of dental services are provided as part of the General Dental Services, funded through the National Health Service (NHS). Patients are registered with a dental practice, and funding is available to facilitate domiciliary care for patients who are resident in nursing homes. However, dental services for care home residents in NI are primarily delivered by the Community Dental Service (CDS), organised across five Health and Social Care Trusts. This is a publicly funded service that provides oral care for a range of patients who have additional needs and where care cannot be delivered within the General Dental Services. The CDS undertakes periodic oral health assessments within care homes across NI, but up to now no published epidemiological data have described the oral health status of care home residents in NI.
The aim of this study was to provide an epidemiological profile of oral health among nursing home residents in NI, and to explore associations between oral health parameters and cognitive impairment.
Materials and methods
Study design
Anonymised oral health assessment data collected by the CDS in care homes across the Belfast Health and Social Care Trust (BHSCT) and the South Eastern Health and Social Care Trust (SEHSCT) were accessed via Data Access Agreements (DAAs) as part of a registered quality improvement project. Data were collected during oral health assessments conducted as part of routine CDS activity. All data were collected by dental officers within the CDS for treatment planning purposes. Consent for examination was obtained by CDS staff prior to the examination taking place, and where necessary family members were involved in discussions. A retrospective epidemiological analysis of oral health assessment records was undertaken for residents in 57 nursing homes. An ethical approval application was submitted to the School of Medicine, Dentistry and Biomedical Sciences Research Ethics Committee at Queen’s University Belfast, but formal ethical approval was not required for secondary analysis of an existing dataset.
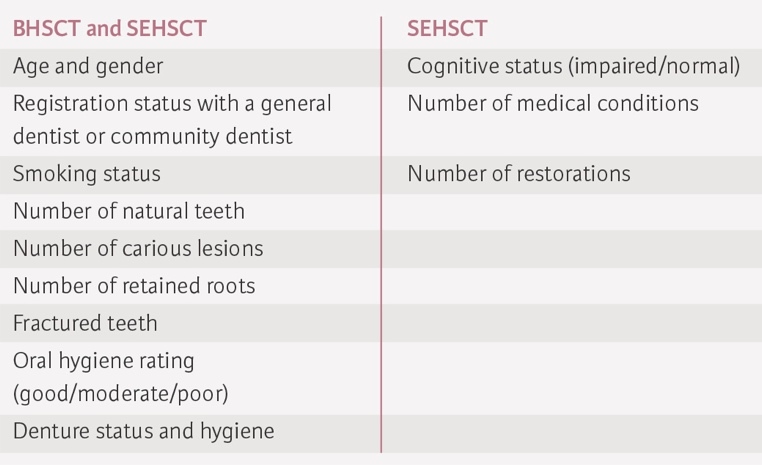
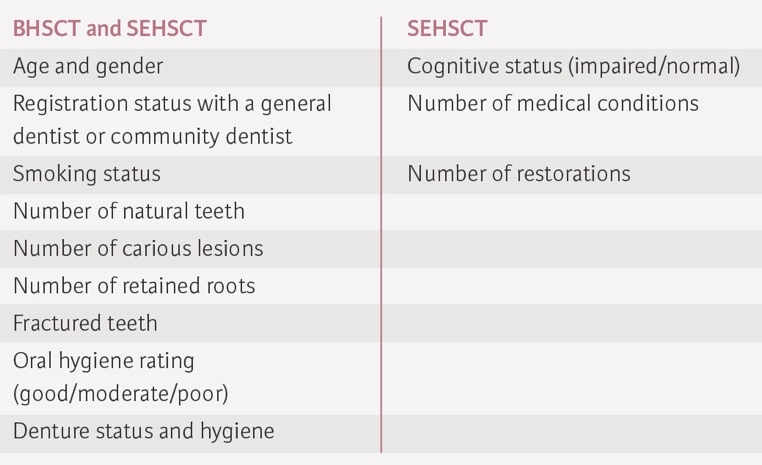
A range of variables were collected for each patient as part of the oral health screening, including general demographics, caries charted on coronal or root surfaces, retained roots, fractured teeth, oral hygiene (graded as good, moderate or poor), and denture status. Retained roots were counted as teeth when qualifying for dentate status and number of remaining teeth. For a smaller subset (SEHSCT; n=381), data were available on cognitive status, medical comorbidities, and number of restorations (Table 1).
Statistical analysis
Data were entered into the IBM Statistical Package for the Social Sciences (SPSS) software. Descriptive statistics summarised population characteristics. Parametric tests examined group differences. Logistic regression explored predictors of dentate status and cognitive impairment. Statistical significance was set at p<0.05.
Results
Demographic characteristics
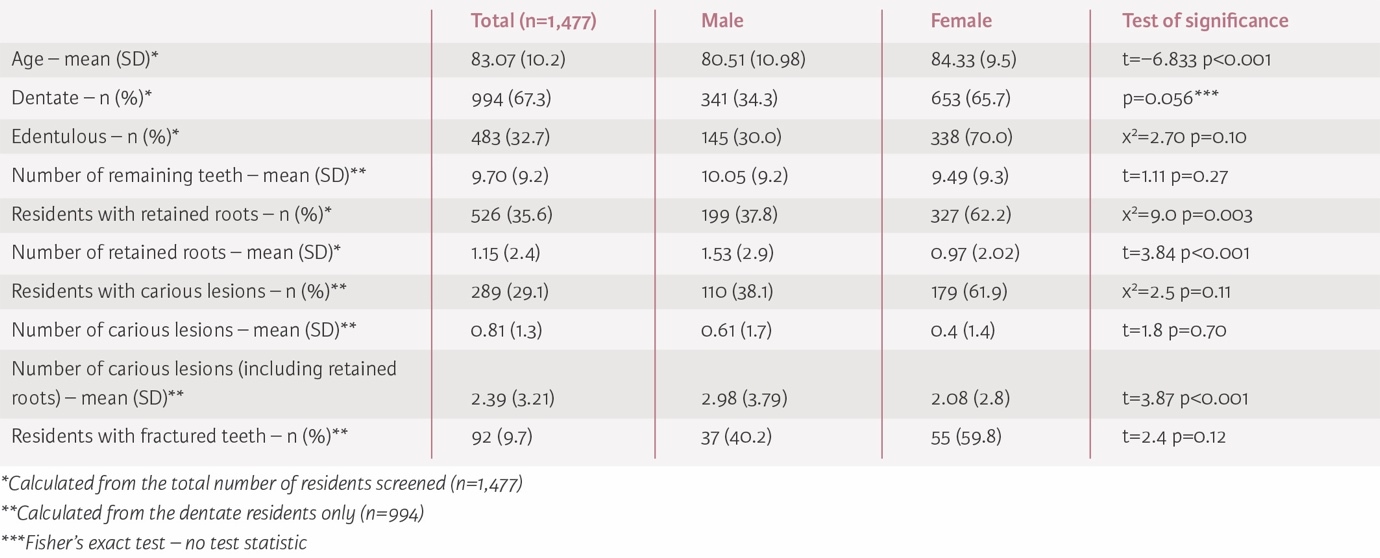
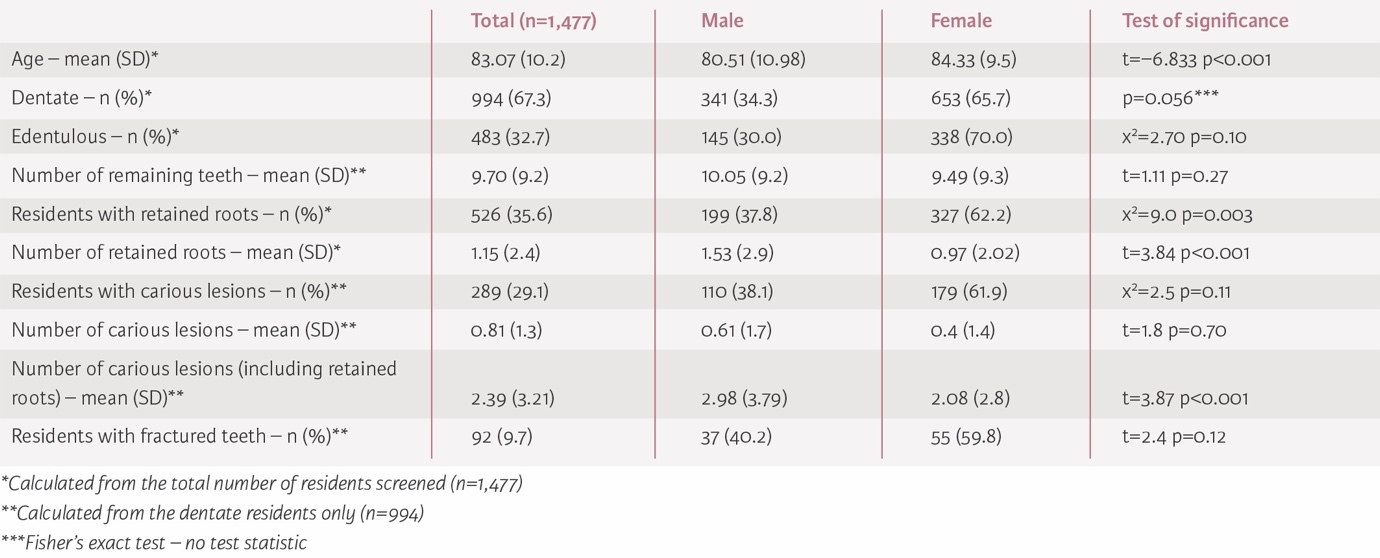
Oral health information was available for 1,477 residents across 57 nursing homes. Within the sample 67.1% were female (n=991), and they had a mean age of 83.07 years (standard deviation [SD] 10.15) (Table 2). The female residents included were significantly older than the male residents (84.3 vs 80.5 years; p<0.001). Registration data (n=765) showed that 67.6% were not registered with a dentist.
Oral health status and natural tooth retention
Residents were classified as dentate when they had one or more visible teeth and/or retained roots. The majority of residents in this cohort were classified as dentate (n=994, 67.3%) using this definition. The mean number of teeth and/or retained roots was 9.7 (SD 9.23; range 1-31) (Table 2).
Age was negatively correlated with the number of remaining natural teeth (r=-0.165; p<0.001). Each 10-year increase in age reduced the odds of being dentate by 27% (odds ratio [OR] 0.73; p=0.017). For every 10-year increase in age, residents had 1.42 fewer teeth (B=-0.142; p<0.001; CI -0.188 to -0.095) and the odds of being dentate were reduced by 16% (Exp(B)=0.840; p=0.003; CI 0.749-0.943). No significant gender differences were found in the number of remaining natural teeth.
Caries and retained roots
Among dentate residents, 29.1% had carious lesions (n=289; mean 0.81; SD 1.3; range 1-14) (Table 2). A large proportion of residents (35.6%) had retained roots in situ (n=527; mean 1.15; SD 2.4; range 0-24). If retained roots were assumed to be carious, the mean number of carious teeth increased to 2.39 (SD 3.21; range 1-24). Male residents had a significantly higher mean number of carious lesions when number of carious lesions and number of retained roots were combined as one variable (t=3.87; p<0.001).
Oral hygiene
Among dentate residents (n=994), 56.3% were recorded as having poor oral hygiene as determined by visual inspection of the oral tissues. No significant gender differences were observed (Table 3).

Denture status
More than half of the residents wore dentures (53.1%, n=609) with the majority constructed from acrylic resin (90.8%, n=553). Among edentate denture wearers, 68.2% (n=210) wore complete upper and lower prostheses.
Cognitive impairment subgroup
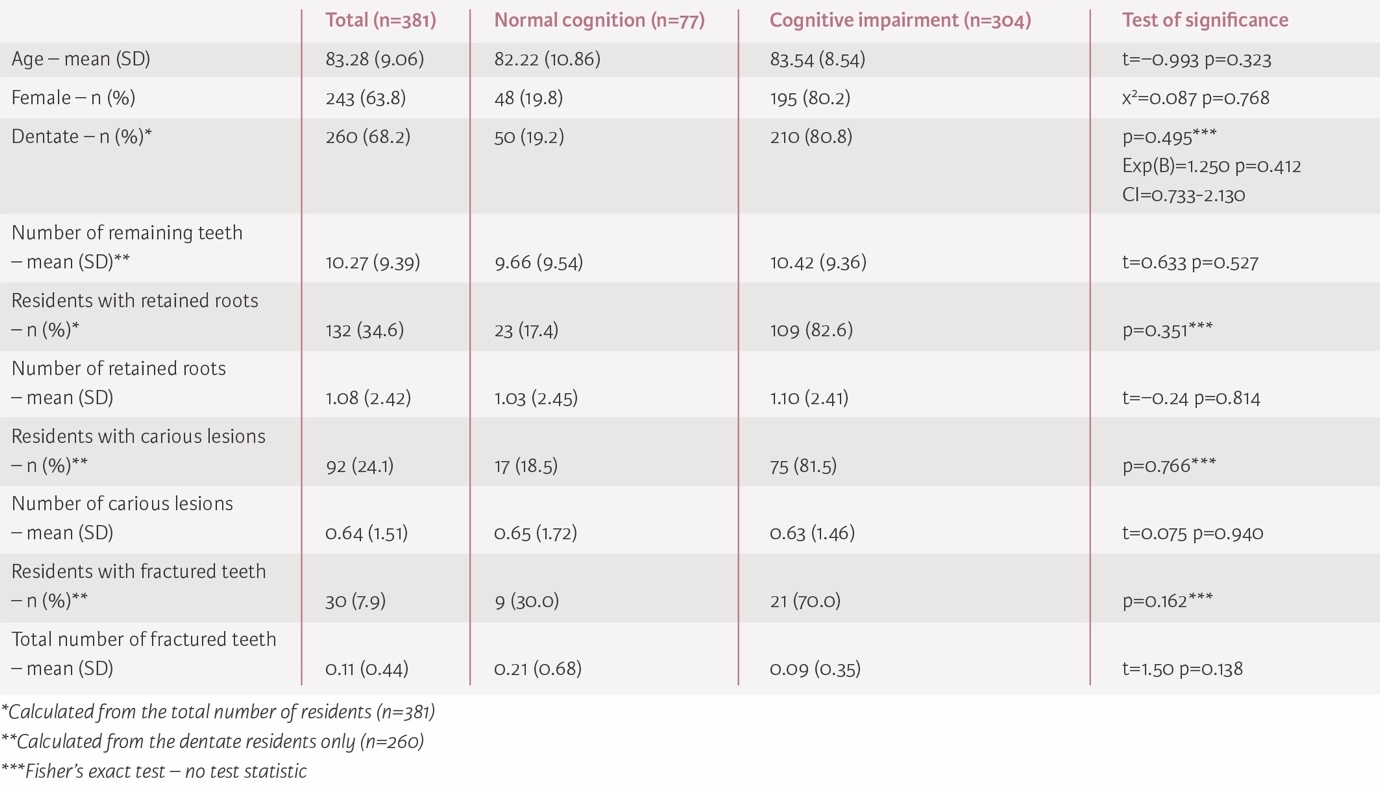
For the subgroup within the SEHSCT with additional information on systemic health (n=381), 79.8% (n=304) had some degree of cognitive impairment recorded. No significant associations were found between cognitive status and number of teeth, caries, retained roots, or oral hygiene (p>0.05) (Table 4). Multivariate logistic regression identified only number of fractured teeth as significantly associated with cognitive impairment (OR 0.55; p=0.026). No other oral variables were significant predictors. Smoking prevalence was low (5.7%), and residents with cognitive impairment were significantly less likely to smoke (p<0.001).
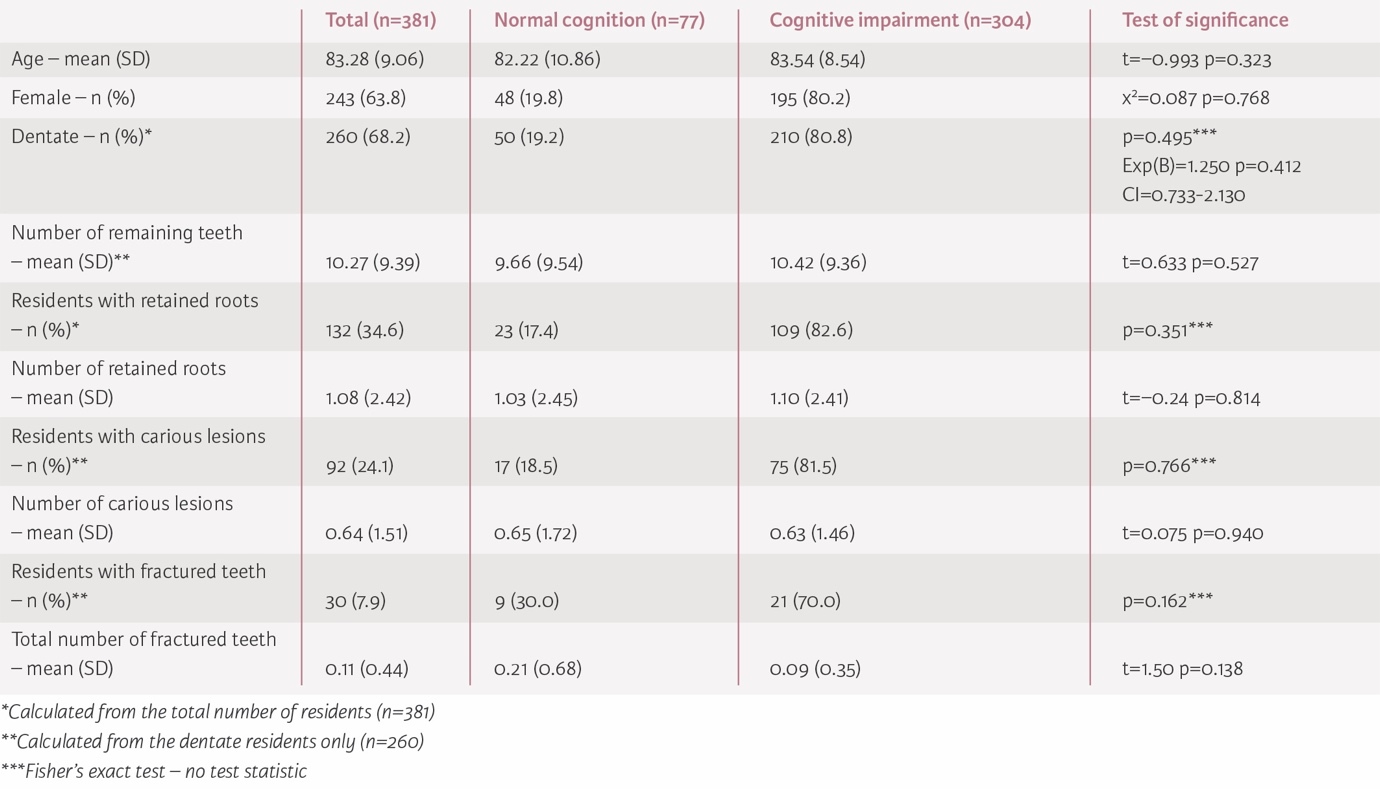
In a logistic regression model, after adjusting for age and setting dentate as the outcome, the residents with cognitive impairment had 25% higher odds of being dentate compared to those residents who were not cognitively impaired (Exp(B)=1.250; p=0.412; CI=0.733-2.130), but this result was not statistically significant. For every 10-year increase in age, the odds of being dentate were reduced by 27% (Exp(B)=0.73; p=0.017; CI 0.57-0.95).
When logistic regression was run in the other direction, with cognitive impairment as the outcome, for every 10-year increase in age, the odds of being cognitively impaired were increased by 20% (Exp(B)=1.20; p=0.204; CI 0.91-1.60), holding gender, number of medical conditions, and total number of remaining teeth constant.
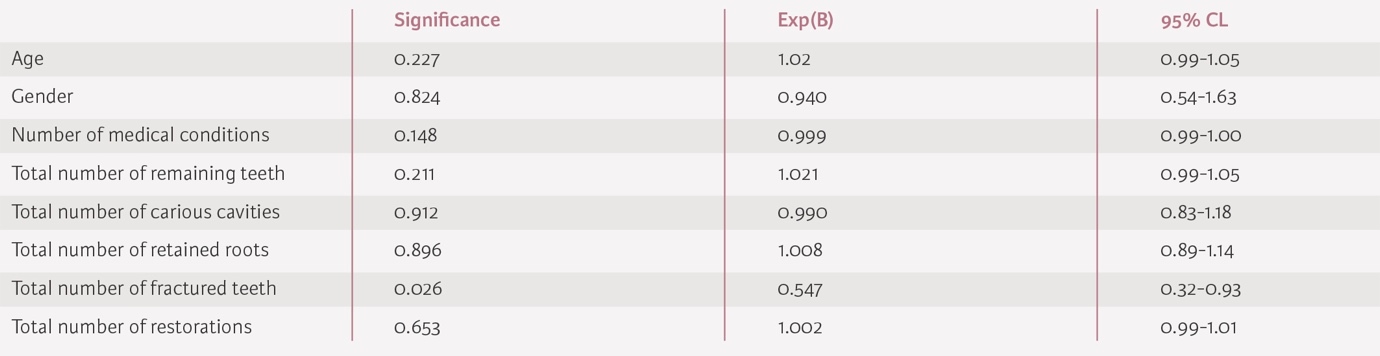
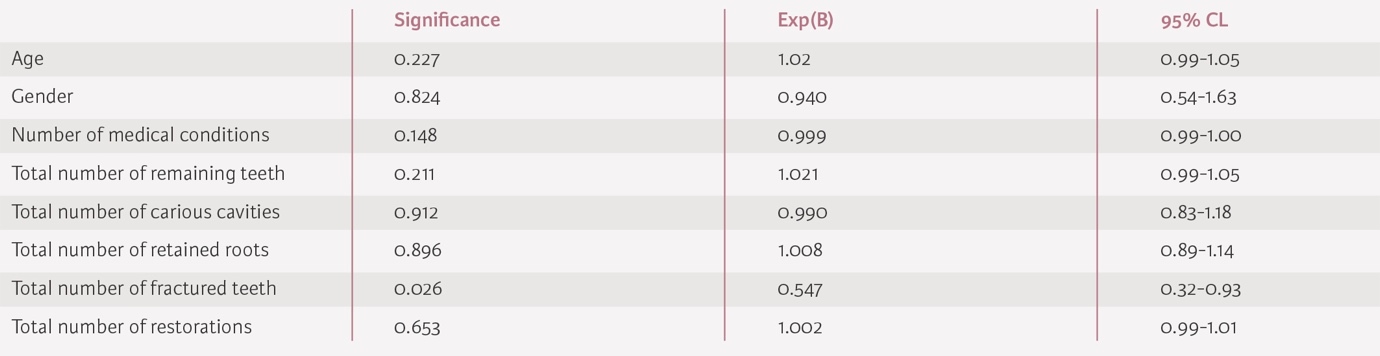
A binary logistic regression (Table 5) was performed to ascertain the effects of age, gender, number of medical conditions, total number of teeth, total number of cavities, total number of retained roots, total number of fractured teeth, and total number of restorations on the likelihood that a resident would have cognitive impairment. The model correctly classified cognitive impairment status in 80% of cases; however, the model was heavily biased against the majority group (residents with cognitive impairment). Further, the only covariate that had any significant association with a resident being cognitively impaired was the total number of fractured teeth. Residents with more fractured teeth had lower odds of being cognitively impaired. Each additional fractured tooth reduced the odds of having cognitive impairment by 45% in this model (Exp(B)=0.55; p=0.026; CI 0.33-0.93). No other variables (age, gender, number of medical conditions, total number of remaining teeth, total number of carious cavities, total number of retained roots, total number of restorations) were significantly associated with cognitive impairment (p>0.05).
Data related to number of systemic comorbidities were available for 98.2% (n=374) of these residents, and 50% had four or more medical conditions. The number of medical conditions ranged from 0 to 13, and the mean number of medical conditions was 3.7. Residents with cognitive impairment had a 10% increase in odds of having four or more medical conditions (p=0.721; CI 0.664-1.807).
Discussion
This large retrospective epidemiological study showed a high burden of dental disease in a vulnerable cohort of our society (approximately 29% of dentate residents had dental caries charted on coronal or root surfaces, and 36% of residents had retained roots in situ). As a result, there was a high need for dental care, including restorative treatment and dental extractions. A significant proportion of the nursing home residents were dentate (67.3%), confirming that residents of nursing homes are retaining their natural teeth into older age. Although cognitive impairment is often associated with poorer oral health, this study did not demonstrate significant associations between cognitive status and most oral health indices. The lack of association may reflect measurement limitations, sample imbalance, or reduced statistical power.
The findings from this study are comparable to the results of other recent epidemiological studies carried out in Belgium that also assessed the oral health of care home residents.8 The mean number of remaining teeth (9.7) in NI was lower than that reported for Belgian nursing home residents (mean 12). However, compared with the general adult population from the 2009 ADHS (93% dentate; mean 25.1 teeth), nursing home residents had markedly poorer oral health. An epidemiological study of the oral health of nursing home residents in Wales (United Kingdom) was carried out in 2010 and used the ADHS as a framework for its methodology. This study also had a large sample of participating residents (n=708), and concluded that the oral health of nursing home residents in Wales was poor, with 72.8% of dentate nursing home residents experiencing tooth decay.9
Research has shown that older people requiring assistance with self-care, such as oral hygiene, have a significantly higher risk of experiencing oral health issues.10 Having poor oral hygiene is known to increase the risk of a person developing dental caries and periodontal disease.11 It is important to increase accessibility to dental health services so that oral diseases can be treated as soon as they are diagnosed. There is increasing pressure on our health and social care services to implement preventive regimes, and to deliver safe and effective treatment where necessary. Promoting oral disease prevention for nursing home residents will prevent unnecessary pain, swelling and hospitalisations related to poor oral health.12 Prevention of oral disease should be prioritised within nursing homes because it spares older people the impact of disease, and preventive services are generally more cost-effective than treatment utilising restorative services.12 The cost of implementing a good oral hygiene regime is small when compared to the expenditure required to manage a serious medical condition such as aspiration pneumonia.13,14 Some oral health and systemic conditions share common modifiable risk factors. The common risk factor approach (CRFA) focuses on tackling risk factors that are common to multiple human diseases to prevent poor general health and reduce health inequalities. It is proposed that targeting periodontal disease will likely be influential in reducing the risk of conditions such as cardiovascular disease and diabetes, and may have implications for other systemic diseases, such as cognitive impairment. A multidisciplinary approach would enable the dissemination of research findings to relevant stakeholders and facilitate the uptake of evidence-based practices in a more efficient and effective manner.15
This is the first epidemiological study of the oral health of care home residents in NI. This study’s main strength is the large sample size, which has allowed the research team to carry out complex statistical analysis to find possible explanations for the observed results. However, given the demographics of the cohort under investigation and the data available, there are a number of limitations to this epidemiological study. Examinations were conducted in non-clinical settings, where there wasn’t access to a dental chair and clinicians used limited illumination. Radiographs were not available, periodontal indices were not recorded, and the team of clinicians were not calibrated, as the data were collected for clinical treatment planning rather than as part of a dedicated research programme. While this represents the challenges of providing screening in the care home sector, these factors would tend to introduce potential measurement bias and therefore it could be assumed that the caries prevalence reported could be underestimated. Furthermore, residents who were unable or unwilling to co-operate with the examination were excluded from the assessment. This has the potential to underestimate the disease burden and introduces further bias. It is also important to note that data collection templates (clinical assessment forms) differed between the Health and Social Care Trusts, and cognitive status and level of comorbidity were only available for a small subgroup of the sample. Rural healthcare settings tend to have a high staff turnover, leading to lack of continuity of dental care, and lack of specialist healthcare providers. The culture of resistance or delay in seeking care is also higher in the rural population.16 Low health literacy can also lead to unhealthy lifestyle behaviours. It is important to recognise that geographic representation was limited to two regional areas. The nursing homes included in this study were all located in the city of Belfast and the surrounding areas. If repeated, this study should include nursing home residents from more rural areas and with a larger geographic spread, in order for the sample to be representative of the population.
Evidence suggests that structured oral health programmes, caregiver training, fluoride use, and daily supervised toothbrushing reduce caries risk in long-term care settings. However, a number of barriers are stated in relation to providing for oral care within nursing homes.17,18 It is important to integrate oral health improvement programmes and preventive strategies into care planning and access pathways.1 Given demographic projections, demand on the CDS will increase. Workforce planning and service redesign must account for rising numbers of dentate, medically complex older adults. Excellent collaboration between the General Dental Services and CDS will be required. There would be value in repeating this work in the post-Covid-19 era with data collected prospectively. This would highlight any current deficiencies in oral care provision among nursing home residents compared to pre-pandemic service levels.
Conclusions
Nursing home residents in NI experience a high burden of untreated dental disease, with the majority now retaining natural teeth into older age. It is clear that the CDS will require prioritisation, investment and development in order to meet the demands of this vulnerable patient cohort, as numbers are projected to increase in the future. Collaboration between the General Dental Services and CDS will also need to be refined.
In the longer term, a heavy emphasis on dental disease prevention is required to reduce dental disease and pressure on dental services. This will require commitment from various stakeholders, to include general medical practitioners, care home nurses, healthcare assistants, and family members of care home residents.