Introduction
Little is known about the oral health of older adults in nursing homes in Ireland. The Irish Longitudinal Study on Ageing (TILDA) is a large, national study that aims to determine current health status and health needs of older people who reside in the community, their social and economic needs, and what the biological and environmental effects of successful ageing are.1 There are limited prior data available regarding the oral health of older adults in Ireland, as the last national survey of the oral health of this population was conducted over 20 years ago.2 However, Wave 3 of TILDA included a dental assessment of adults over 50 who live in the community.3
Action 33 of Smile Agus Sláinte, Ireland’s oral health policy, specified the development of a nationally agreed set of core criteria to assess the oral health of patients at each World Health Organization (WHO) indicative age, including those aged 65 and older.4 TILDA has helped to provide more information on older adults in the community. However, there is a paucity of information regarding adults of a similar age in residential settings. Action 34 aims to develop a programme for pathfinder studies that will initially focus on residential centres and vulnerable people.3,4 In Ireland, approximately 20% of nursing homes are publicly funded Health Service Executive (HSE) facilities, approximately 3.7% are run by not-for-profit organisations, and the remaining 77% are run by private providers.5
The Dental Treatment Services Scheme (DTSS) in Ireland currently entitles eligible adult medical card holders to an annual examination, teeth cleaning, extractions, and two fillings per year. Additional treatments such as dentures and periodontal treatment are available to some patients.6 Austerity measures introduced in 2010 resulted in funding for this Scheme being cut from €62m to €10m from 2010 to 2015, causing severe restrictions in restorative and preventive dentistry, which are still largely in place today.7 A subsequent exodus of dentists from the DTSS has created access issues nationally for patients, and further pressure on the HSE dental services.8 For those in residential care, this may cause further barriers to accessing dental care. Additionally, there may be variation in their oral health needs, their ability to manage their own oral health, and in support and training in this area from staff.9
The Modified Oral Status Survey Tool (MOSST) was developed by Trinity College Dublin, the Trinity Centre for Ageing and the Life Course in Intellectual Disability (TCAID), and Dublin Dental University Hospital, in partnership with adults with intellectual disabilities (ID) for use on the Intellectual Disability Supplement of the TILDA study (IDS-TILDA).10 The MOSST covers seven concepts that indicate oral status and oral function. It was developed to be quick, acceptable, robust and administered by non-dental professionals (such as nurses and healthcare assistants), as well as by dental professionals, without the use of an assistant or scribe.10,11 The aim of the MOSST is to collect data based on the following concepts: number of functional tooth units; aesthetics (presence of the front 12 teeth); denture wear; number of teeth in each arch; cavitated teeth; gum condition; and, oral cleanliness. The MOSST-Self Report Supplement (SRS) aims to collect data on selected aspects of oral healthcare utilisation, oral health behaviours (home care), and oral health related-quality of life (OHRQOL).10,11 The MOSST can be used for research, or to inform service planning and policy, but is not designed to be used to assess the dental needs of individuals or to replace appointments with a dental professional.10,11 It was hypothesised that the MOSST could be used by dentists to determine the oral health status of people who reside in nursing homes in Ireland.
The aim of this pilot study is to assess the use of the MOSST in private nursing homes in Leinster (Dublin, Kildare, Wicklow, Carlow, Kilkenny, Laois, Longford, Meath, Westmeath, and Wexford). The objectives of this pilot study are to:
-
Trial the use of the MOSST by a dentist in the nursing home population in Ireland to determine its appropriateness and identify challenges with dental research in this population.
-
Provide initial data on the oral health status of participants based on an intra-oral exam.
-
Provide initial data on dental service use and OHRQOL based on a questionnaire.
Methods
The examiner was a dentist with experience of working with vulnerable adults. Training and calibration of the dentist on the MOSST and MOSST-SRS were completed in March 2024, with a combination of online and in-person sessions facilitated by Dr Caoimhin Mac Giolla Phadraig and Katrina Byrne (Trinity College Dublin). The dentist achieved an inter-rater agreement Kappa statistic result of 1.00, and therefore a very good strength of agreement with the gold standard examiner. Ethical approval for the study was granted by Trinity College Dublin’s Faculty of Health Sciences Research Ethics Committee in December 2024. This included a data protection impact assessment.
Convenience sampling from private nursing homes in Leinster was undertaken. Each of the facilities was contacted by email or phone call, and an accompanying letter. Gatekeepers for each facility who did not provide direct clinical care to nursing home residents were identified. Adults were targeted via their nursing homes, and consent forms and participant information leaflets were given to each person selected for inclusion. Patients aged 65 and older living in nursing homes in Leinster were included in this study. The study was explained by the gatekeeper, and anyone who expressed interest, or was able to express interest, in participation was then met by the dentist, who went through the participant information leaflet and consent form.
The dentist who undertook the examination determined if informed consent could be taken on the day, and some participants were excluded on the day as they could not provide consent in any form (for example, some patients were bed bound and non-verbal, and could not indicate whether they understood the study). Many potential participants were excluded by gatekeepers and nursing staff due to conditions such as advanced dementia. A gatekeeper was required by the Faculty of Health Science, Trinity College Dublin to be “someone in an administrative role, not directly responsible for clinical care”. In order to participate, informed consent was required. Those who could not provide consent were not included.
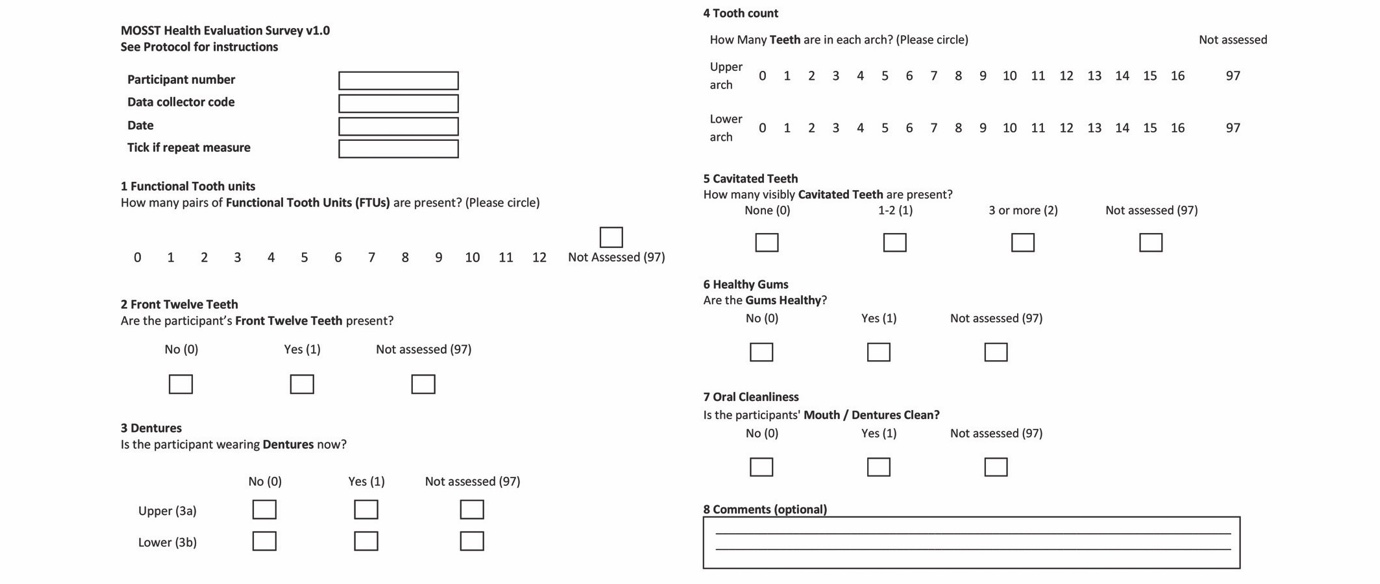
Data collection was undertaken by an Irish Dental Council-registered dentist, using a dental mirror, head torch, and personal protective equipment (PPE). The MOSST and the MOSST-SRS were used to gather data for all participants who could provide consent (Figure 1). Every participant was given a verbal summary of findings, including discussion of care options, and a written letter similar to that used in the TILDA study recommending urgent, soon or routine care need. Need for dental care was also discussed with their care team in the nursing home.
The MOSST-SRS was used to investigate specifically selected aspects of oral healthcare utilisation, oral health behaviours, and OHRQOL for each participant via multiple choice questions.
.jpeg)
Results
Five nursing homes were visited, which in total housed 366 residents. Gatekeepers for each nursing home aided in identifying residents interested in participating and who were able to provide informed consent. While 86 people were presented for examination, the final sample for the oral examination totalled 78 (21.3%) people, as seven could not provide informed consent and one declined to participate.
Of the 78 people who participated in the MOSST, 26 were male and 52 were female. The mean participant age was 80.6 years. All participants were given feedback on their oral health needs and advised whether they should see their dentist routinely, soon or urgently. No participants were identified as having urgent dental needs, such as acute infection or suspicious lesions.
The 21.3% of the total population who were able to participate likely represent those more capable of personal oral healthcare. Therefore, while these results may be an underestimate of need, the initial findings were as follows.
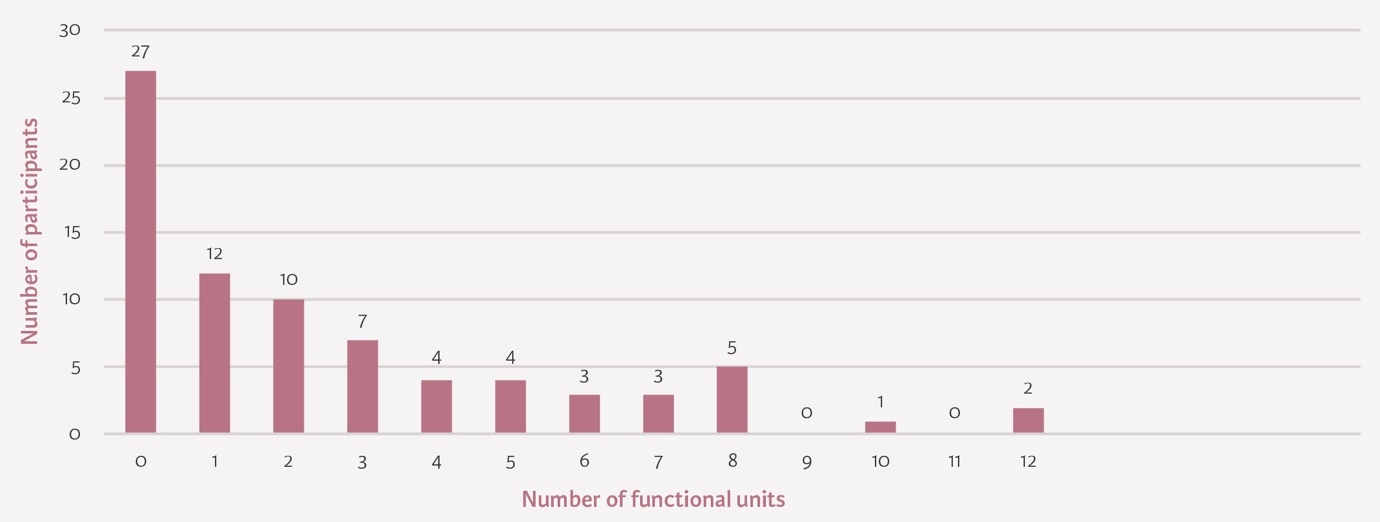
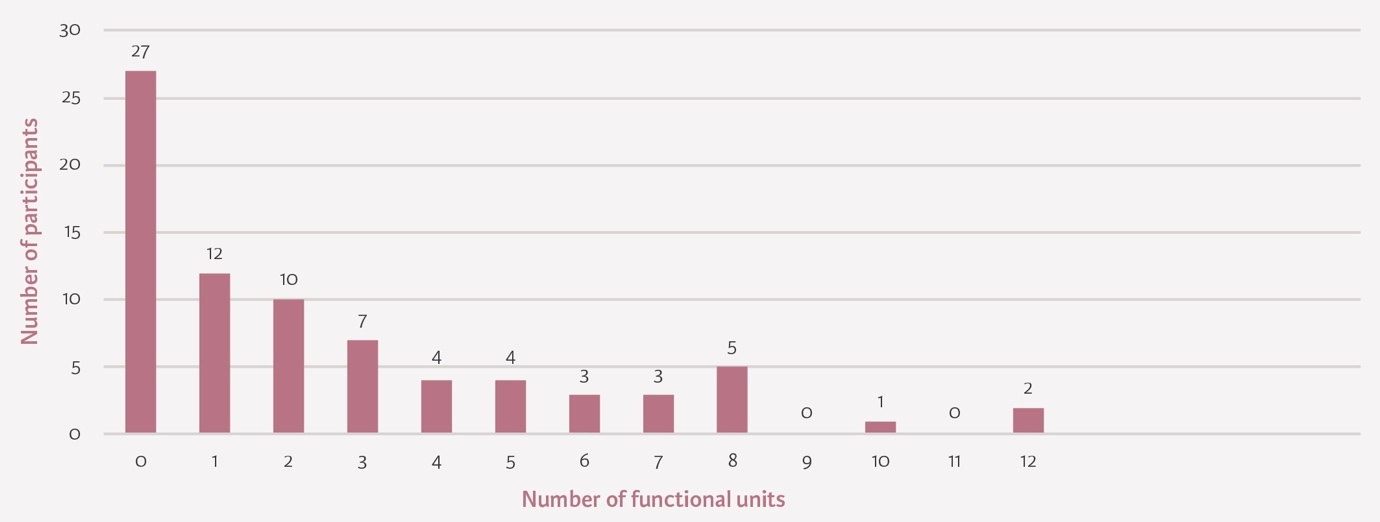
The first part of the MOSST assessed the number of functional units of each participant, which may consist of natural or prosthetic teeth. A molar pair counts as two functional units, while a pre-molar pair is one. There was a lot of variation in numbers of functional units between participants (Figure 2).
The next part of the MOSST focused on aesthetics, looking at whether each participant had 12 front teeth present, either natural or prosthetic. From this sample, 56 people out of 78 had 12 front teeth present, which is over 70% (71.8%). Participants were then investigated for denture use, and recorded as wearing an upper or lower denture only if they were wearing one at the time of examination. Over 35% (n=28) of residents were wearing an upper denture and 23.1% (n=18) were wearing a lower denture.
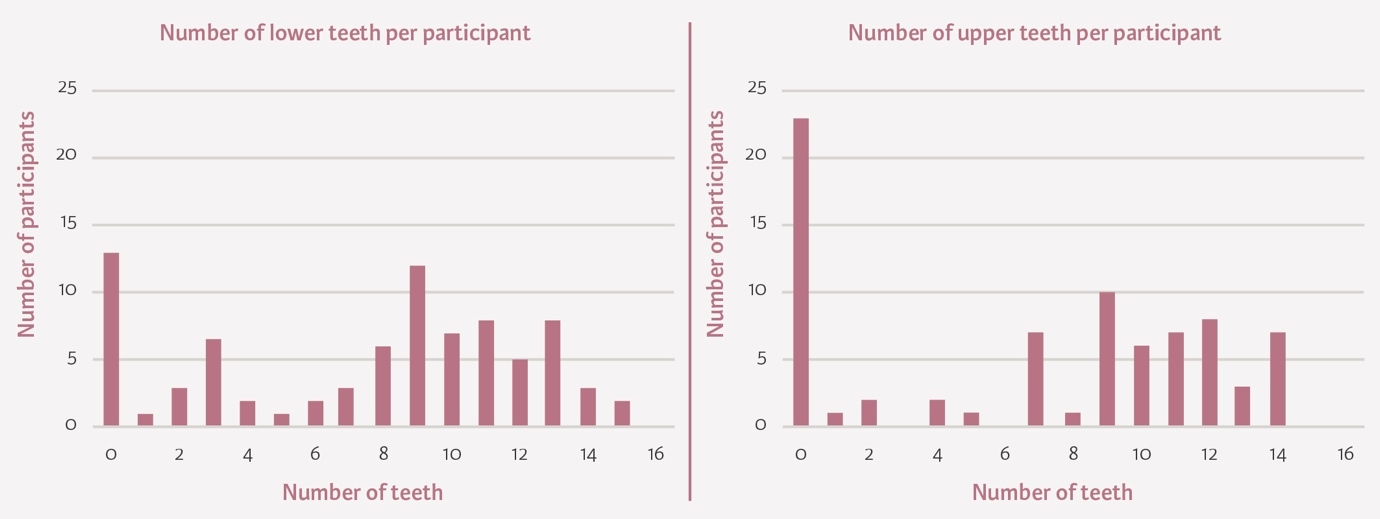
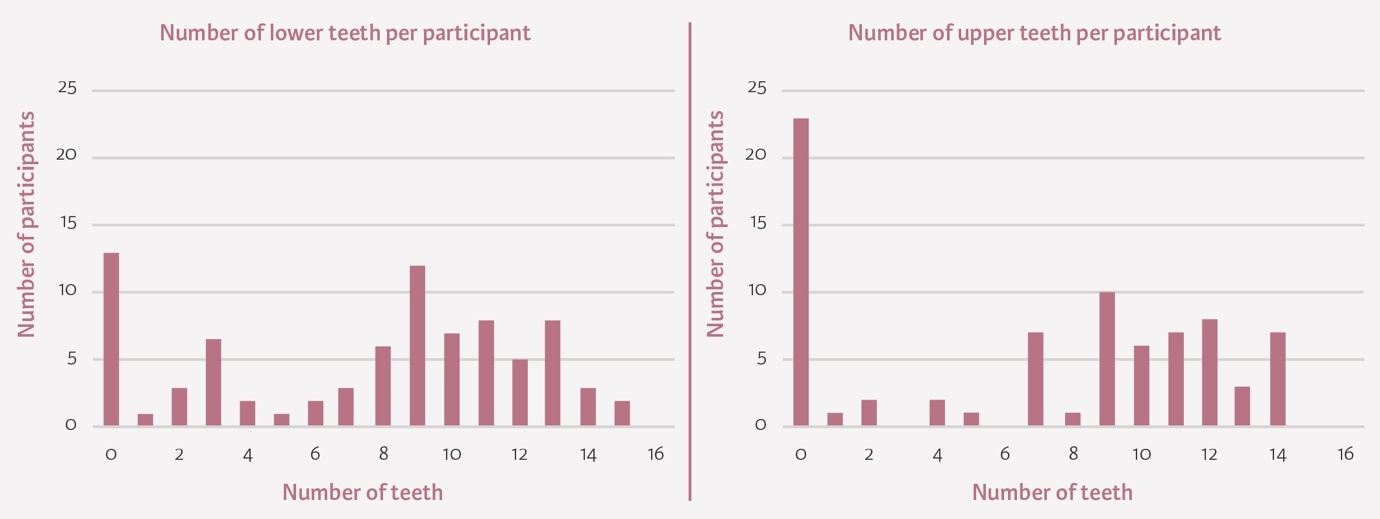
Dentures were then removed and the number of teeth per arch recorded. The mean number of teeth per participant in the upper arch was 6.86, and for the lower arch it was 7.81 (Figure 3).
In terms of cavitated teeth present, over 60% (64.1%) had no visibly cavitated teeth present, although 19% of participants had three or more cavitated teeth. Over 70% of the sample (n=60) had healthy gums, and 59% (n=46) had clean mouths/dentures.
Participation in the questionnaire was more varied, as some participants did not answer certain questions. Four participants required some assistance to answer questions.
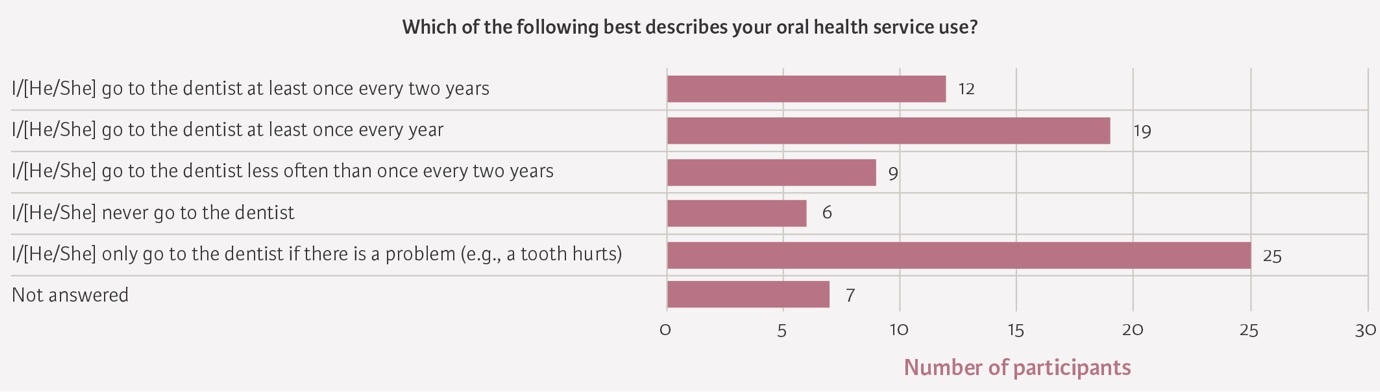
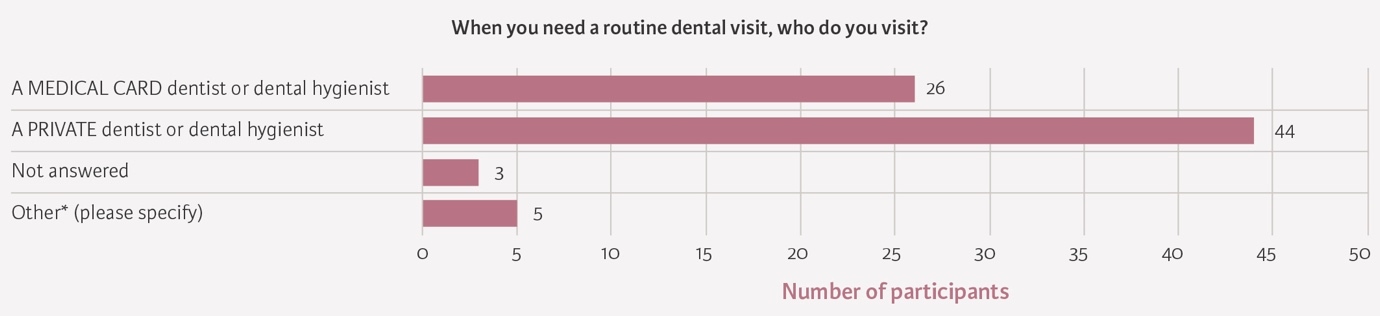
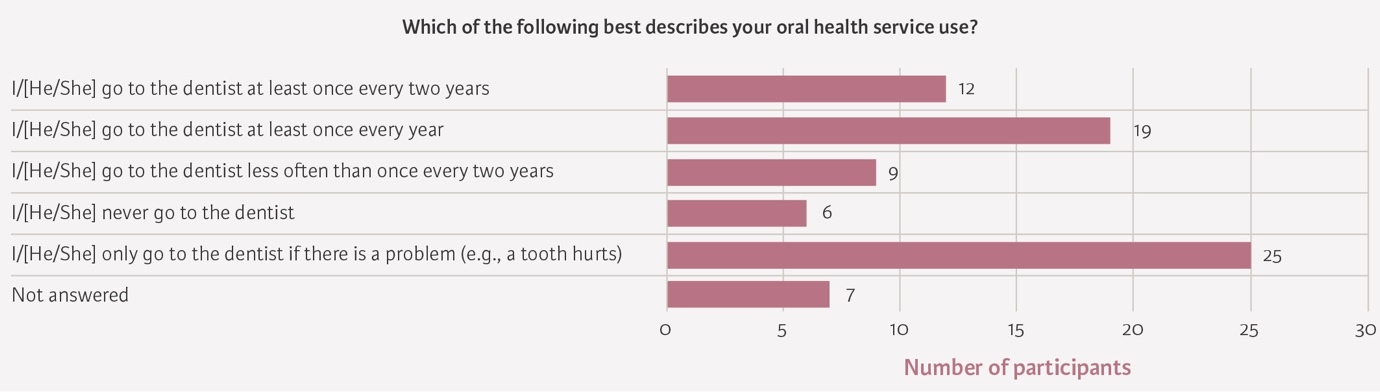
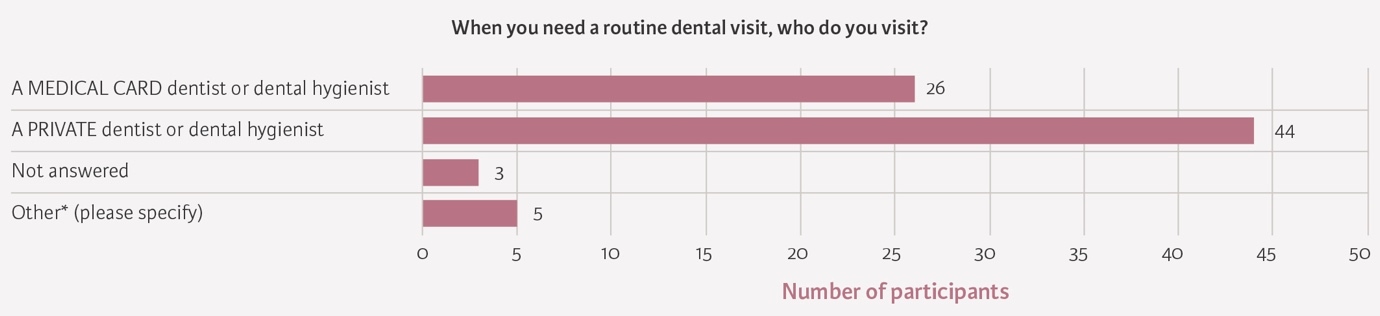
When asked about their oral health service use, there was a lot of variation in terms of regularity of attendance, with over 30% of participants only going to see the dentist if they have a dental problem (Figure 4). The majority of participants (56.4%, n=44) stated that when they need a routine dental visit, they attend a private dentist or hygienist, and 26 participants (33.3%) stated that they attend a medical card dentist (Figure 5). When asked if they needed additional measures for routine dental treatment such as restorations, 17 participants did not answer this question, but the majority (75.6%, n=59) answered that they only needed local anaesthesia.
In response to being asked about barriers to accessing dental care, 65 participants reported no difficulty in accessing dental treatment. Three people stated that there was a long waiting list to see their dentist, one participant reported difficulty accessing dental treatment, and one person responded that their dentist did not have the facilities to treat them. The majority of patients (84.6%) found it easy or very easy to get a dental appointment.
Most participants (75.6%, n=59) reported that they were happy or very happy with their smile. Over 90% of patients (91.0%, n=71) reported no oral pain in the last week. The majority of participants (75.6%) reported no difficulty chewing, though 16.7% of participants (n=13) reported difficulty chewing with some types of food and 6.4% (n=5) with all types of food.
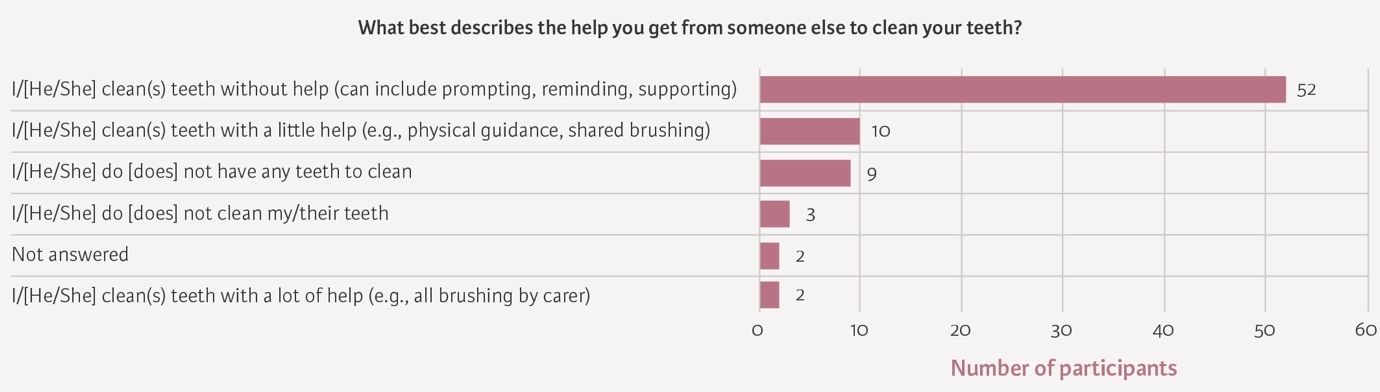
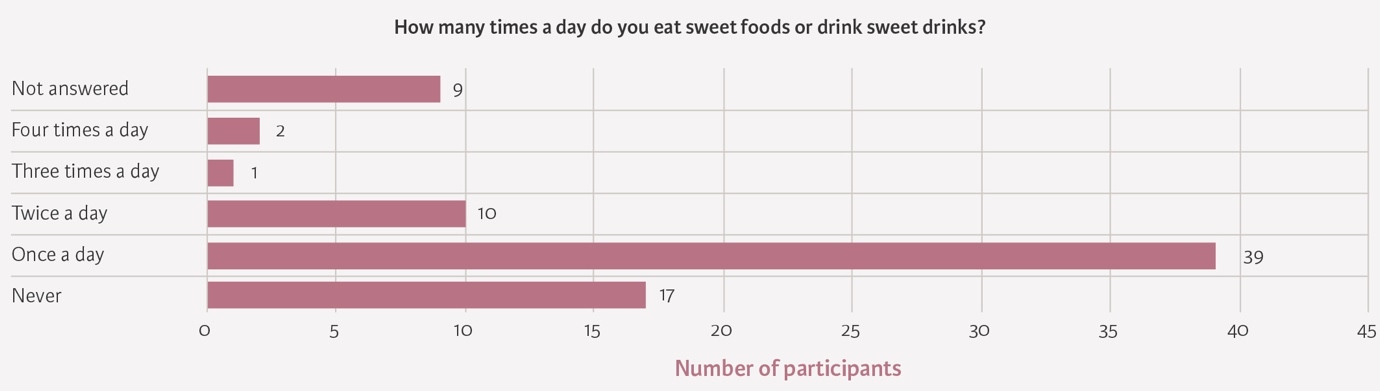
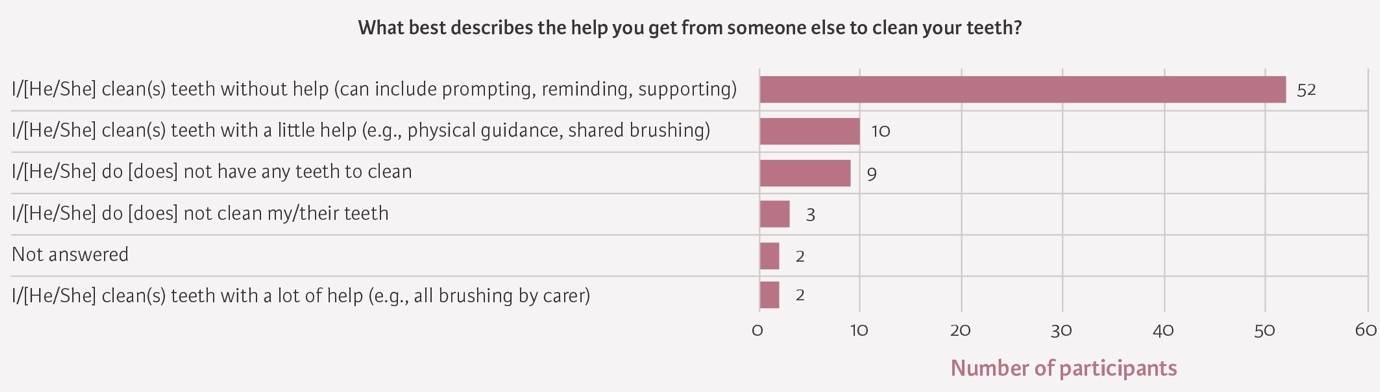
In terms of oral health behaviour, most participants reported brushing their teeth at least once a day (76.9%, n=60), and the majority of participants (66.7%, n=52) reported that they could clean their teeth without assistance, while 7.8% (n=10) reported needing a little help (Figure 6). Most participants did not have a mouthcare plan (93.6%, n=73). Over 60% of participants (n=52) consumed sugary sweets or drinks at least once a day (Figure 7).

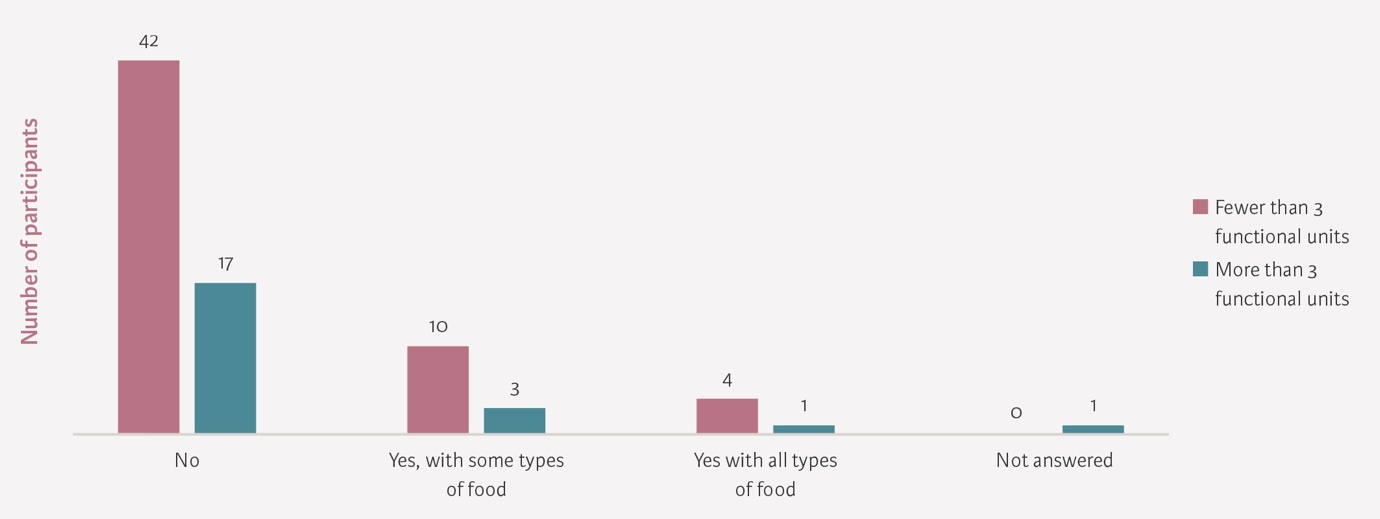
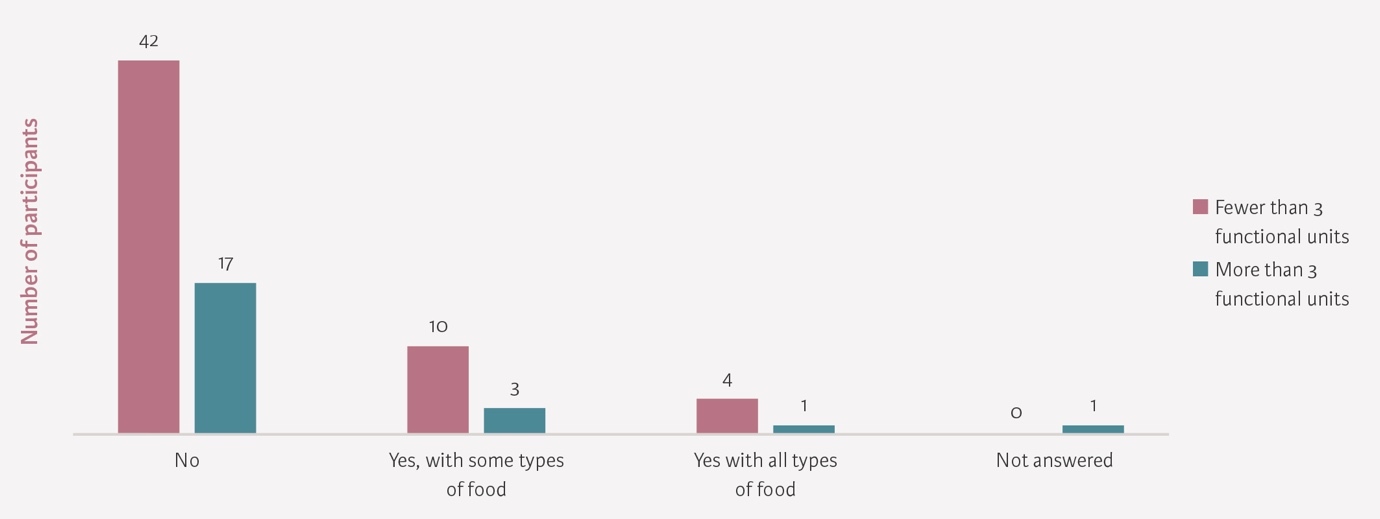
The majority of participants (n=59) reported no difficulty chewing, despite over 20% (21.8%) having fewer than three functional units present (Figure 8). Having 10 tooth contacts (20 occluding teeth) is considered to be a minimally functional dentition.3
Discussion
This pilot study illustrates the difficulties of research in the nursing home population. Large numbers of people were not able to provide informed consent and participate in the MOSST. It is important to note that the profile of the population sample was included simply to give initial pilot data on the oral health of care home residents able to participate. This may inform methods in future, larger studies. However, due to the limitations outlined, such as the limited number of the target population who could provide informed consent, this cannot be seen to be representative of the general population of care home residents in Ireland.
The results relating to oral health status are reflective only of those in private nursing homes who could provide informed consent and were willing to participate in this study, and are therefore highly likely to be an underestimate of need. The gatekeepers identified barriers, such as advanced dementia, to providing informed consent. Less than 25% (21.3%) of potential participants could provide informed consent and were willing to participate. In the pilot, the examination was conducted by a dentist with extensive experience of providing dental care for vulnerable adults. Non-dental professionals report low confidence and a lack of training in dealing with the oral cavity in this population.12,13 This has important implications for further epidemiological research in this area. It would also be useful to include some data around the use of services by people in care homes in Ireland, to provide more context for the dental needs of this population.
Although not currently suitable for providing reliable and valid data at the population level, for those able to consent, the MOSST was easy to use in this population and beneficial in that it can be used by dentists and non-dentists after the completion of training. It provided a good overview of the oral health status of this consenting population, with functional units, cavitation, denture use, and number of natural teeth included. Number of teeth or functional units has previously been reported as being directly related to chewing.14,15
This relationship was not observed here, and 42% of participants had no difficulty with chewing, despite 20% having fewer than three functional units present. Additionally, the majority of participants (75.6%) felt happy about their smile. This may be attributable to the disability paradox, whereby patients’ perceptions of personal health, well-being and life satisfaction are often discordant with their objective health status and disability.16 A similar lack of correlation was found with the number of cavitated teeth and reported pain. This may be due to natural changes to tooth structure associated with ageing, but may also illustrate a difference between expected need and dental service use. As this is pilot study data, this could again be explored further with a properly powered sample. It should also be highlighted that nursing homes may want to have emergency protocols in place for the management of pain and infection, and may want to work with individuals and families to ensure that residents have appropriate oral care plans on file, which would necessitate a dental consultation.
Limitations and suggestions for further study
The MOSST was originally validated for adults with intellectual disabilities as part of the IDS-TILDA supplement, comparing favourably with dentist-performed examinations.10,11 In this pilot, the MOSST was completed by a dentist to explore its feasibility and acceptability in a nursing home population. Because this setting differs from the original validation population in terms of age, cognitive status, and oral health needs, further work is warranted to examine whether the MOSST can be reliably and accurately used by non-dentists, such as nurses or carers, to identify residents requiring dental referral. A subsequent validation phase could therefore compare MOSST assessments conducted by trained non-dentist staff with independent dentist examinations using standard clinical indices, and estimate inter- and intra-rater reliability for use in long-term care settings.
As the MOSST-SRS was designed for people with intellectual disabilities, some of the questions may not be necessary for this population and others could be added or modified to be more appropriate for the nursing home population.10,11 This could be done by using Public and Patient Involvement (PPI) prior to future research.10 Examples of questions that could be considered for inclusion are ‘When did you last see a dentist?’ and ‘How long have you been in this nursing home?’. This could be important for this population, as their engagement with or use of dental services may have changed dramatically when transitioning from living at home to a nursing home. Question 4 regarding barriers could be modified to include issues faced by nursing home residents. Oral health service use question 3 on whether adjuncts to local anaesthetic are needed prior to a restorative treatment could be considered for omission as it may be more geared towards people with intellectual disabilities. There may be other pertinent questions identified for potential inclusion, and further research, perhaps using service use data, may be needed to identify more suitable and relevant questions for this population. The prevalence of dementia in the population examined was unknown and could have impacted the ability of participants to accurately self-report during the MOSST-SRS, potentially influencing the results. Incorporating a brief cognitive screening tool, such as the Mini-Cog, prior to the MOSST-SRS could help to ensure the reliability of the results.17
Conclusions
-
This pilot study trialled the MOSST and MOSST-SRS in the private nursing home population of Leinster, and found that the MOSST was relatively easy to use for those who could consent. However, the small proportion of the population who were willing and able to be examined restricts the validity and generalisability of the results across the population as a whole.
-
The MOSST-SRS would benefit from being tailored to this population more specifically, through PPI.
-
This was a convenience sample, and only reflects those in private nursing homes in one province of Ireland, who were able to provide informed, valid consent (21.3% of the targeted population).
-
The majority of this sample population (75.6%) were happy with their appearance and function despite huge variations in functional units and numbers of natural teeth.
-
It is important for nursing homes and their staff to know of emergency dental protocols and accessible practices, and more research may be needed to investigate these knowledge levels in the community.
Funding
The authors have no funding sources to declare.
Data availability statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Author contributions
Conceptualisation of the project: Darshini Ramasubbu, Brett Duane
Data collection: Darshini Ramasubbu
Data interpretation: Darshini Ramasubbu, Jonathan Lewney
Writing of the original draft: Darshini Ramasubbu, Jonathan Lewney, Brett Duane
Final approval of the draft and agreement for accountability: Darshini Ramasubbu, Jonathan Lewney, Brett Duane
Ethical approval
Ethical approval for the study was granted by Trinity College Dublin’s Faculty of Health Sciences Research Ethics Committee in December 2024 (ref. 240610). This included a data protection impact assessment.