Introduction
Class II division 1 malocclusion (II/1M), with prominent upper incisors and an increased overjet, affects 25-30% of children and adolescents.1–3 It is commonly associated with bullying, incisor trauma, low self-esteem, and poor oral health-related quality of life (OHRQoL) in the child and associated family.4–8 There is, however, variation in the related perception by child and parent of the aesthetic orthodontic treatment need.9 Growth modification of II/1M with a functional appliance has been shown to improve dentofacial aesthetics, self-esteem, OHRQoL, and perception of aesthetic orthodontic treatment need of both child and parent.5,8–13 The twin block appliance (TBA), or a modification thereof (MTB), is a commonly used and well-tolerated functional appliance for initial correction of II/1M (Phase 1); this aims to achieve a Class I incisor relationship and is typically followed by fixed appliances (Phase 2) to complete treatment.14,15 Treatment with a TBA or MTB principally influences the lower face through combined effects on the orofacial soft tissues and muscles of mastication, producing dentoalveolar and skeletal changes.16 Maximum benefit is reaped during the pubertal growth period, and the soft tissue effects of TBA/MTB treatment may be monitored in an accurate and non-invasive manner, using three-dimensional (3D) imaging.17,18
The aim of this study was to assess the impact of initial correction (Phase 1) of II/1M with an MTB on children and their parents compared to untreated children with II/1M and their parents. The primary outcome was:
- child-reported OHRQoL.
The secondary outcomes were:
-
child-reported self-esteem;
-
child self-perception of the aesthetic orthodontic treatment need;
-
3D soft tissue facial images;
-
family QoL;
-
parental perception of the child’s OHRQoL; and,
-
parental perception of the child’s aesthetic orthodontic treatment need.
Materials and methods
Ethical approval was granted from the Clinical Research Ethics Committee of the Cork Teaching Hospitals.
Study design
This was a non-randomised clinical intervention study.
Setting, participants and eligibility
This study was undertaken in a State-funded orthodontic service in the Republic of Ireland (RoI). The following inclusion and exclusion criteria were adopted:
Inclusion criteria
-
Children aged 11-14 years with good oral health, an overjet of at least 7mm, and about to commence orthodontic treatment with an MTB;
-
children with an overjet of at least 7mm awaiting treatment; and,
-
a parent of each child willing to participate.
Exclusion criteria
-
Previous orthodontic treatment; and,
-
presence of a craniofacial syndrome.
Intervention
Informed consent was obtained from each participant and/or their parent. At the start (T1) and end of MTB treatment, or approximately one year after the initial visit for the control group (T2), each participant completed two validated questionnaires: the Child Perceptions Questionnaire for children aged 11 to 14 years (CPQ11-14) and the Child Health Questionnaire Child Form (CHQ-CF45). These assessed OHRQoL and health-related quality of life (HRQoL), respectively.19,20 Each participant also self-assessed the perception of aesthetic orthodontic treatment need using the Aesthetic Component of the Index of Orthodontic Treatment Need (AC-IOTN), and had a 3D facial soft tissue image recorded at rest (Appendix 1).21 At the same timepoints, the accompanying parent of each participant completed AC-IOTN and the Parental–Caregivers Perceptions Questionnaire (P-CPQ) with respect to their child; details of these outcome measures are provided in Appendix 2.21,22 Details of bite registration, appliance design, and instructions regarding wear are provided in Appendix 3. Participants wearing an MTB were followed until a Class I incisor relationship was achieved.
Sample size
The sample size was calculated on the primary outcome of OHRQoL; using data from Johal et al.,6 a sample size of 30 subjects per group (15 females and 15 males) was required to detect a clinically significant difference of 35% in the OHRQoL between the MTB group and the control group, with a power of 80% and p<0.05. To allow for a drop-out rate of up to 50%, we aimed to recruit 60 subjects per group.23
Statistical analyses
Comparisons of patient demographics were made using analysis of variance (ANOVA) and Chi-square tests. ANOVA was used for comparisons of CPQ11-14, P-CPQ, CHQ-CF45, and 3D soft tissue facial changes at T1 and T2 between groups, and paired t-tests for comparisons within both groups. For AC-IOTN, within- and between-group comparisons were made using Bowker’s test for symmetry and Fisher’s exact test, respectively. Associations between OHRQoL measures, AC-IOTN, and 3D soft tissue facial change were performed using ANOVA. All statistical analyses were performed in SAS (Version 9.4, Cary, North Carolina, USA). The significance level was p<0.05.
Results
Study participants
MTB group
Sixty participants (31 males; 29 females) and a parent of each consented to the study. The non-compliance rate was 30% (11 males; seven females). The final sample comprised 42 patients (20 males; 22 females), with a mean age of 12.6 years (standard deviation [SD] 1.0), and a parent of each. For all 42 participants and their parents, all questionnaire instruments were available at T1 and T2; 3D images at both timepoints were available for 37 patients (18 males; 19 females). Treatment duration with the MTB was on average 8.5 months (range 5-12).
Control group
Forty-seven participants (22 males; 25 females) with a mean age of 12.5 years (SD 0.7), and a parent of each agreed to participate. At T2, data were available for 35 subjects (15 males; 20 females)/parent pairs. At T2, 26% (seven males; five females) did not re-attend. Participants in the control group were recalled on average at 11 months (range 9-13).
Comparisons of groups at T1 and T2
At T1, mean age and gender were similar between groups (p>0.05), but mean overjet was 1mm greater in the MTB group (MTB group: 10.2mm (SD 1.7); control group: 9.2mm (SD 1.5); p<0.01). At T2, the only difference between groups was a significant reduction in the mean overjet (MTB group: 3.1mm (SD 1.3); control group: 8.7mm (SD 1.8); p<0.0001).
Study outcomes
All comparisons between the MTB group and control group were adjusted for age, gender, and overjet.
Child perception of their oral health-related quality of life in MTB and control group at T1, T2, and T2 versus T1
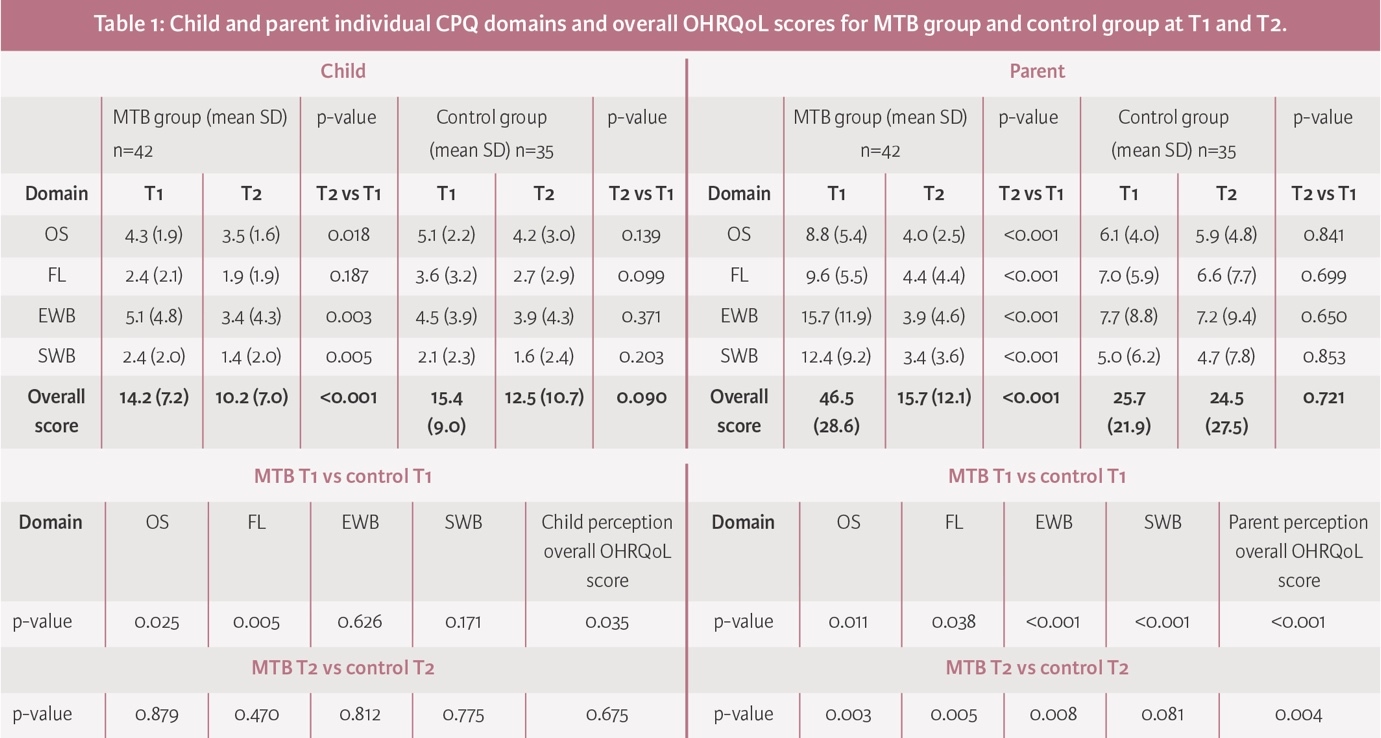
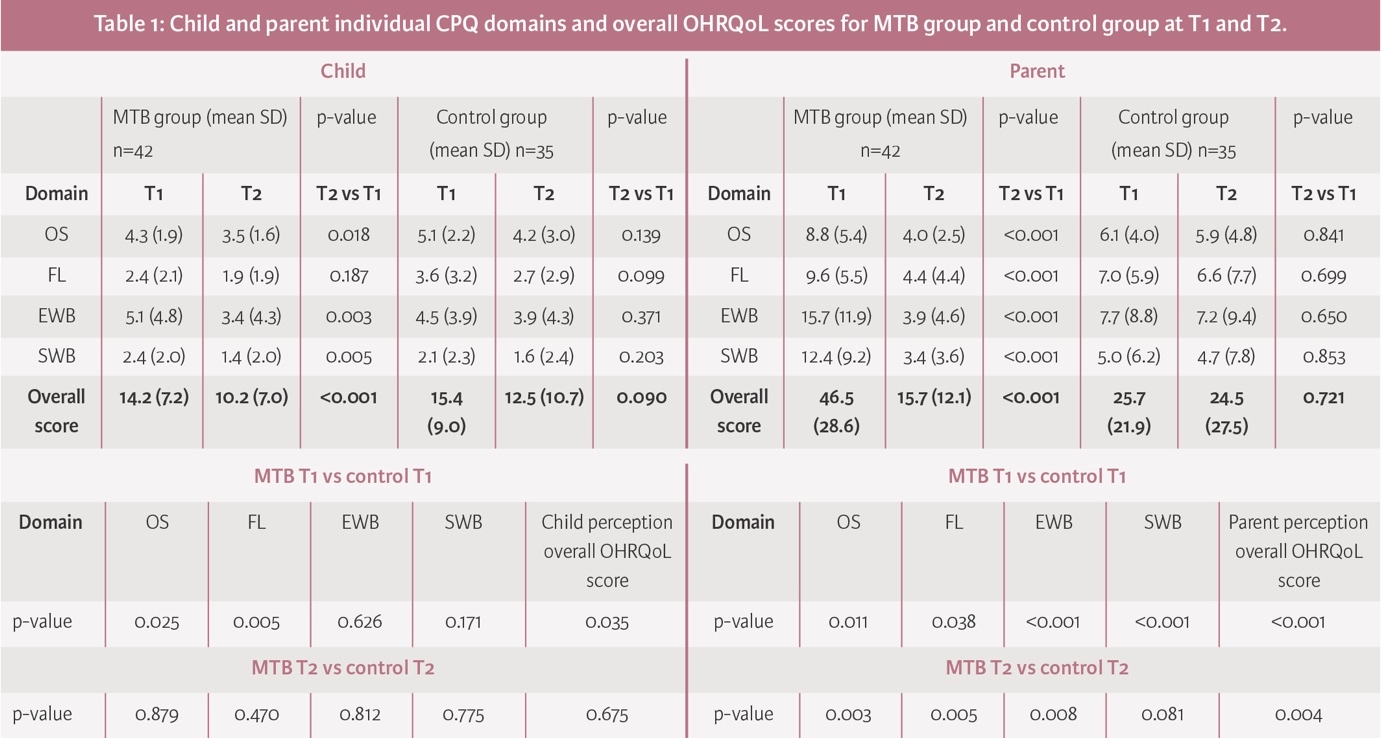
At T1 for both groups (MTB vs control), the self-perceived overall OHRQoL score measured using CPQ11-14 was poor (higher scores), but it was significantly poorer in the control group compared to the MTB group (p<0.035); this was true for the domains ‘Occlusal Symptoms’ (OS) (p<0.025) and ‘Functional Limitations’ (FL) (p<0.005), but not for the domains ‘Emotional Well-being’ (EWB) and ‘Social Well-being’ (SWB). Surprisingly, at T2 there was no significant difference between groups for the overall OHRQoL score, or in any of the four domains. When T2 and T1 were compared, in the MTB group, there was a significant improvement in the overall OHRQoL score (p<0.001), and in the OS (p<0.018), EWB (p<0.003), and SWB domains (p<0.005). In the control group, between T2 and T1 there were no significant differences (Table 1).
Self-esteem of the MTB and control group at T1, T2, and T2 versus T1
There was no significant difference between or within groups over time (p>0.05).
Child perception of aesthetic orthodontic treatment need in MTB and control group at T1, T2, and T2 versus T1
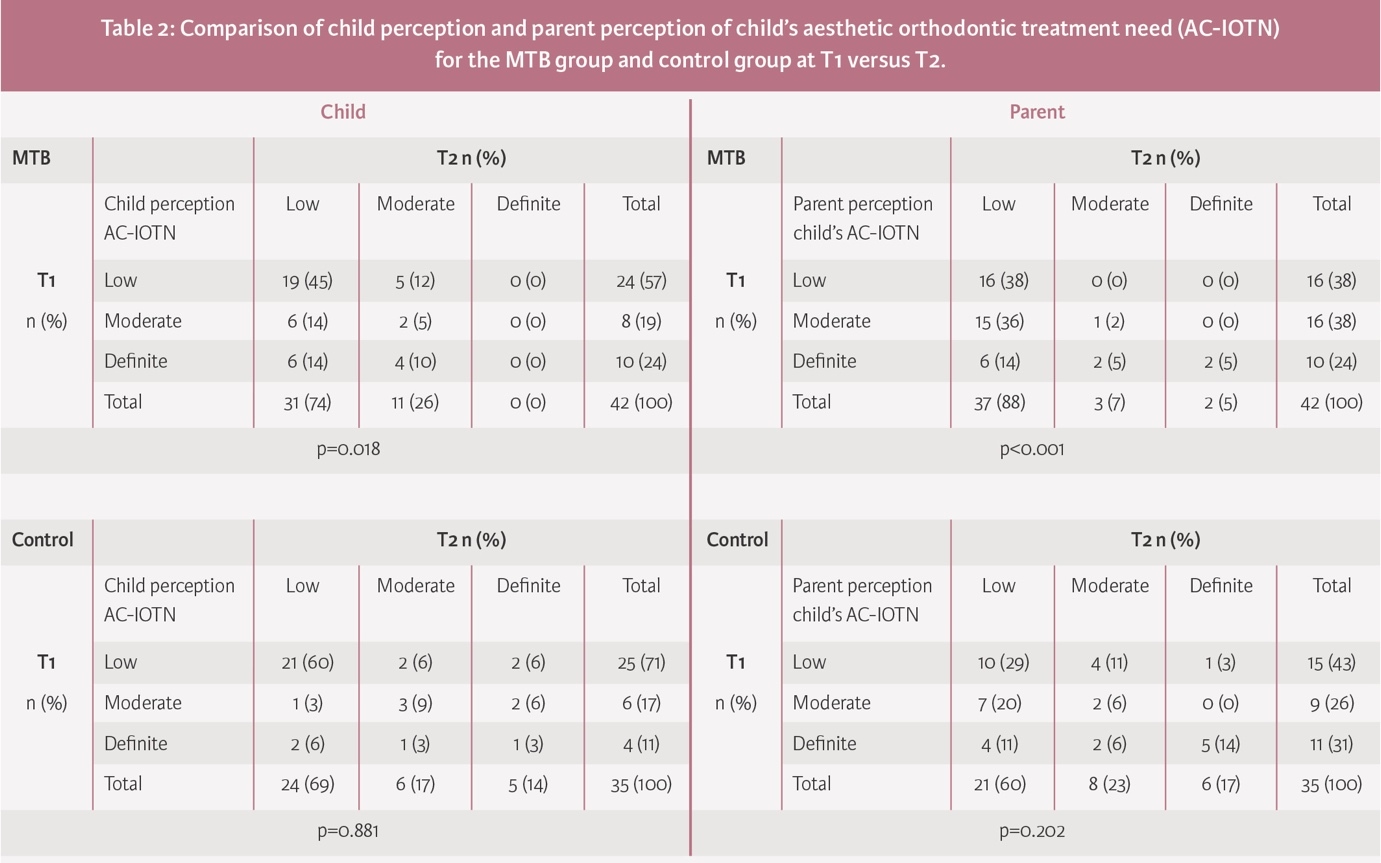
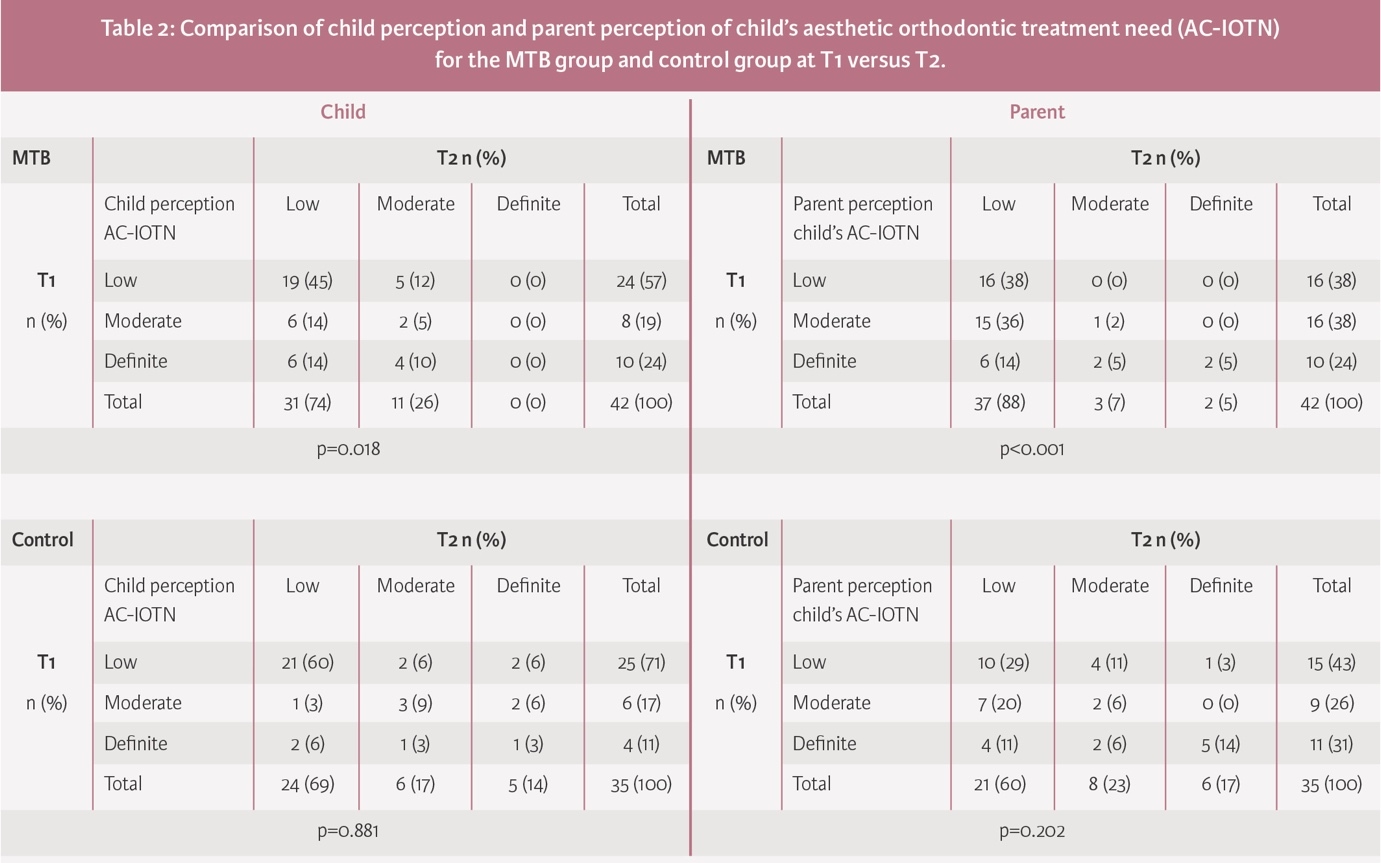
At T1, 43% of participants in the MTB group reported a moderate or definite AC-IOTN compared to 28% at T2 (p=0.018). In the control group, a moderate or definite AC-IOTN was identified at both timepoints (T1: 28% and T2: 21%; p=0.881) (Table 2).
Parent perception of their child’s OHRQoL in MTB and control group at T1, T2, and T2 versus T1
At T1, parents of children in both groups perceived their child to have a poor overall OHRQoL score; for the MTB group, this was rated almost twice that reported for the control group (46.5 vs 25.7; p<0.001). Parents perceived a significant difference in all four domains (OS, FL, EWB, and SWB). At T2, in the MTB group, there was a significant improvement in the parent’s perception of their child’s overall OHRQoL (p<0.001). There was no significant change in the control group (25.7 vs 24.5; p=0.721). When comparing both parental groups at T2, the parents of the control group had a significantly poorer rating of their child’s overall OHRQoL score across all domains (p<0.004) (Table 1).
Parent perception of their child’s AC-IOTN in MTB and control groups at T1-T2
At T1, 62% of parents of the MTB group perceived a moderate or definite AC-IOTN, and at T2 this had reduced to 12% (p<0.001). At T1, 57% of parents of the control group perceived a moderate or definite AC-IOTN, and at T2 this reduced to 40% but was not significantly different (p=0.202) (Table 2).
Family quality of life in MTB and control groups at T1, T2, and T2 versus T1
At T1, the mean family QoL score in the MTB group was significantly poorer (13.6; SD 9.9) than the mean family QoL score in the control group (6.9; SD 7.5, p=0.0008). Following Phase 1 treatment with an MTB, the family QoL improved substantially (13.6 (SD 9.9) to 2.4 (SD 2.3); p<0.0001), but was no different in the control group (6.9 (SD 7.5) to 5.2 (SD 8.3); p=0.221). The mean scores at T2 were significantly different between groups (p=0.0024).
Child perception and parent perception of their child’s OHRQoL in MTB and control group at T1 and T2
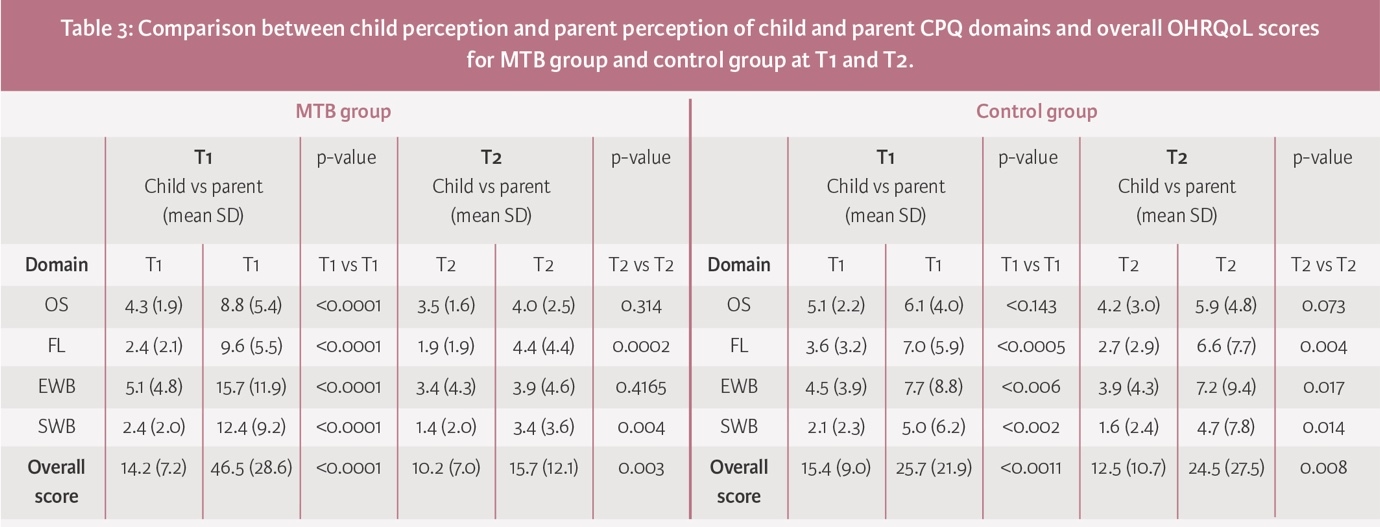
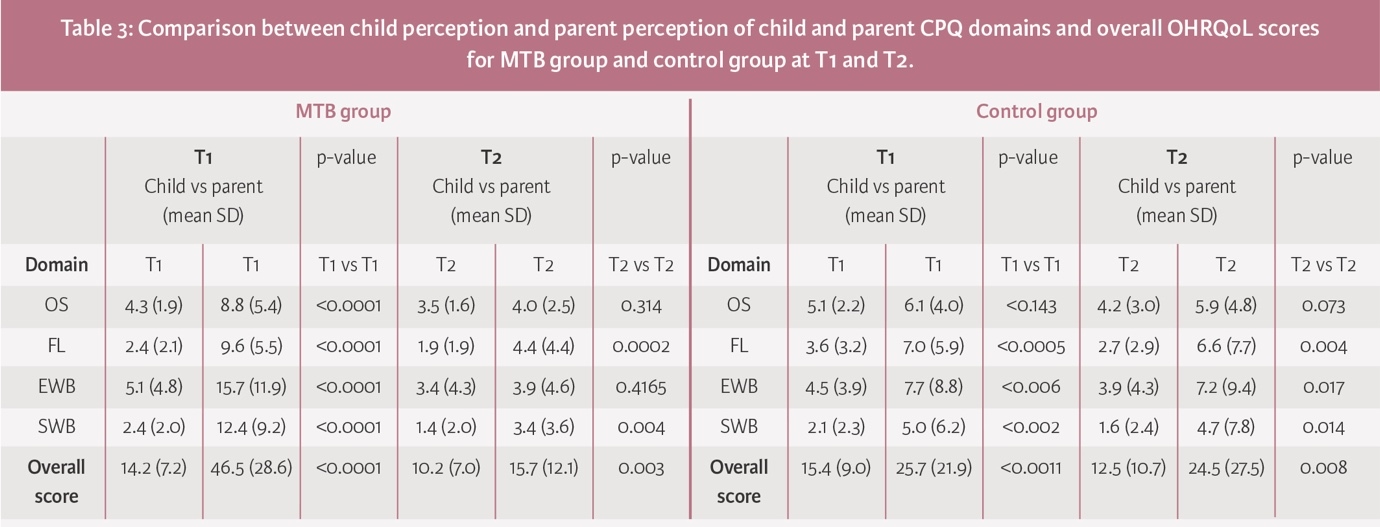
At T1, in the MTB group, there was a significant difference between self-perception and parental perception of the child’s OHRQoL. Parents perceived that II/1M had a more negative impact on their child’s OHRQoL than the child did; this was true both overall and in each of the domains of OHRQoL (p<0.0001). At T2, although children and parents reported a significant improvement in overall OHRQoL, parents still rated this worse than children (child: 10.2 (SD 7.0) and parent: 15.7 (SD 12.1); p=0.003) (Table 3).
Similarly, in the control group, parents’ perception of their child’s overall OHRQoL at both timepoints was significantly poorer than their child’s perception (p<0.0011 and p=0.008) (Table 3).
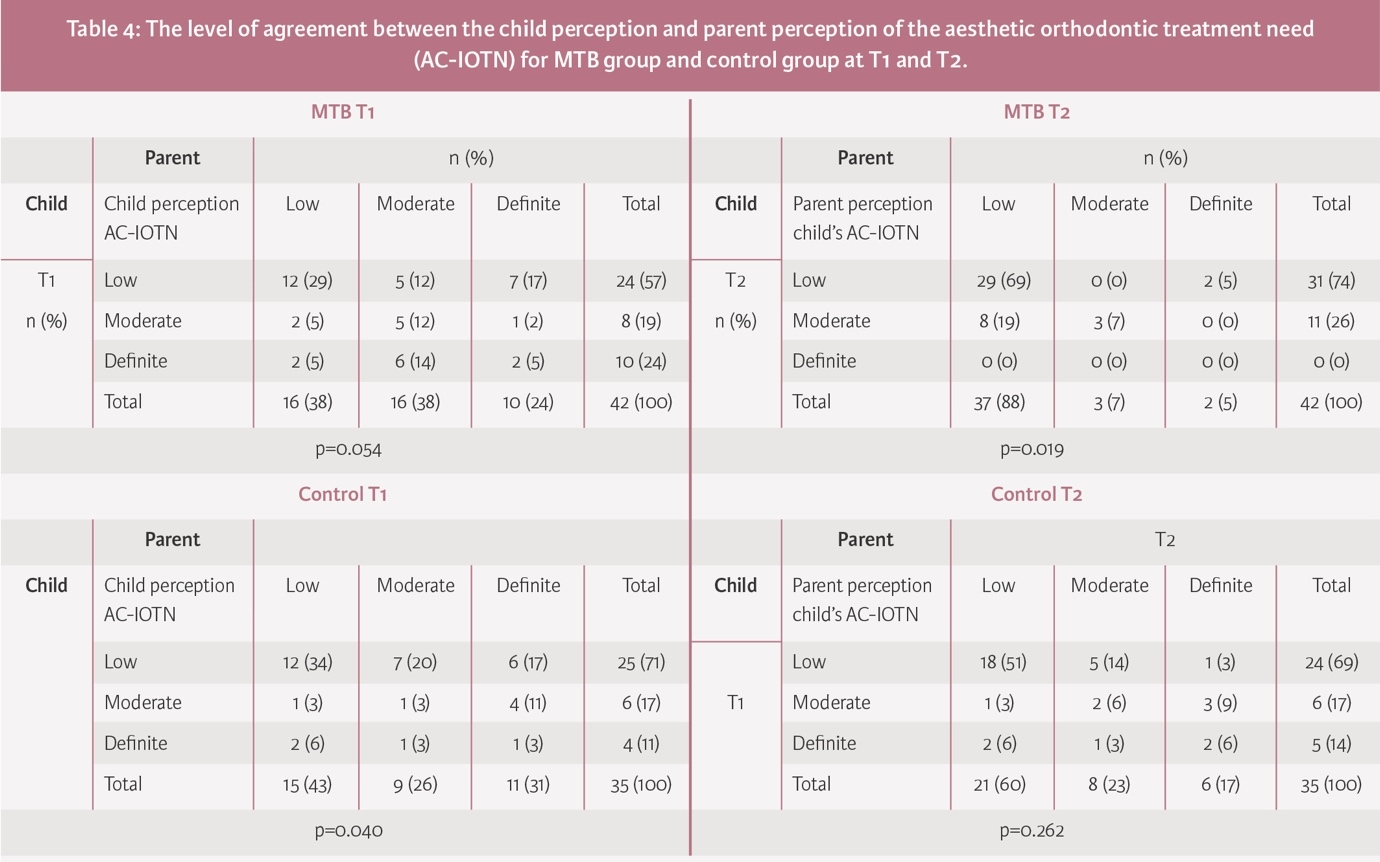
Child and parent perception of AC-IOTN in MTB and control group at T1 and T2
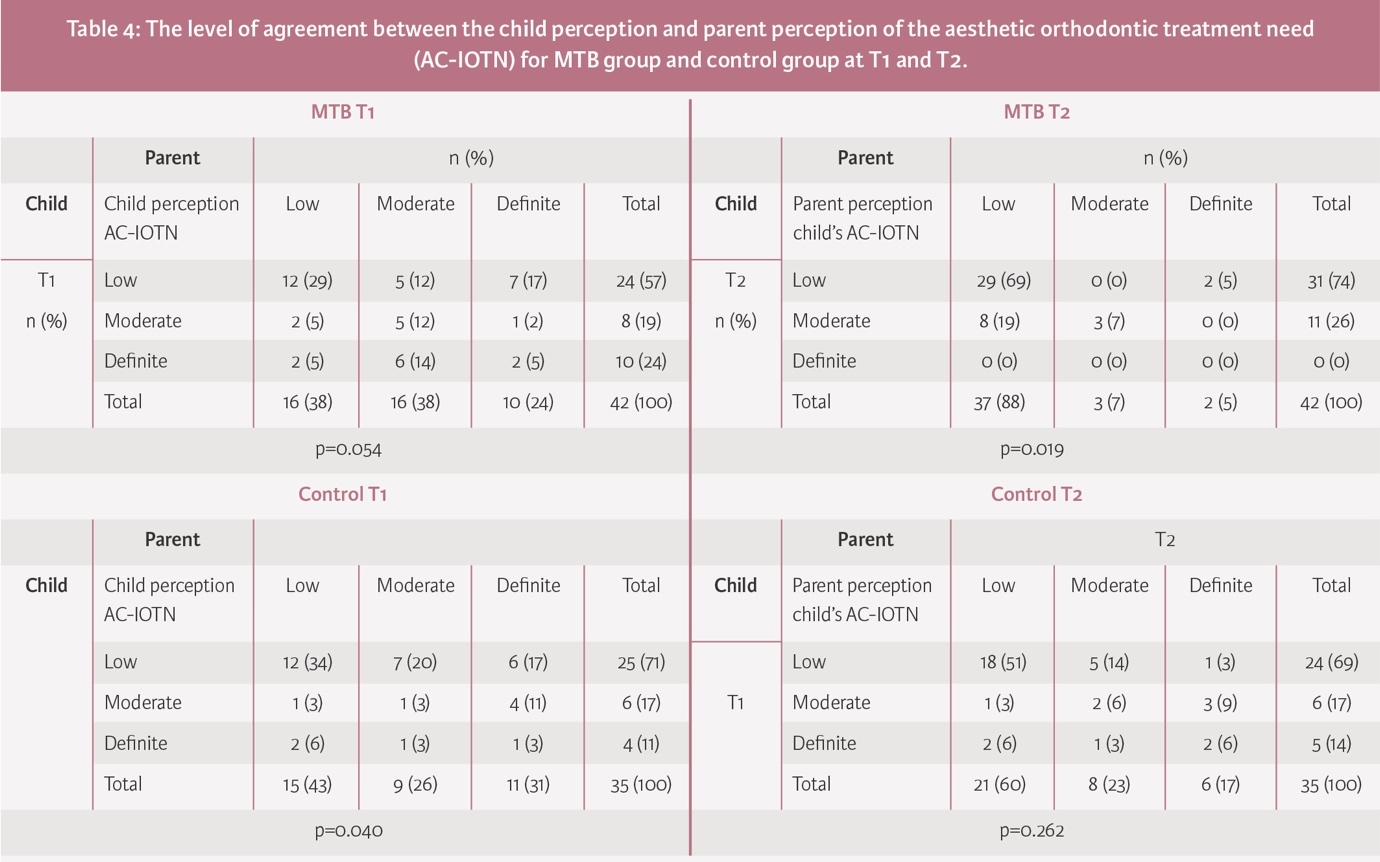
At T1, in the MTB group, 46% of children and parents perceived a similar aesthetic orthodontic treatment need (p=0.054). At T2, following MTB treatment, 69% of children and parents perceived a low treatment need, and although 19% of children perceived a moderate need, their parents perceived a low need (p=0.019) (Table 4).
At T1, in the control group, 40% of children and parents perceived a similar aesthetic orthodontic treatment need (p=0.040). At T2, 51% of children and parents perceived a low treatment need; 14% of children and 17% of parents perceived a definite need, although this difference was not significant (p=0.262) (Table 4).
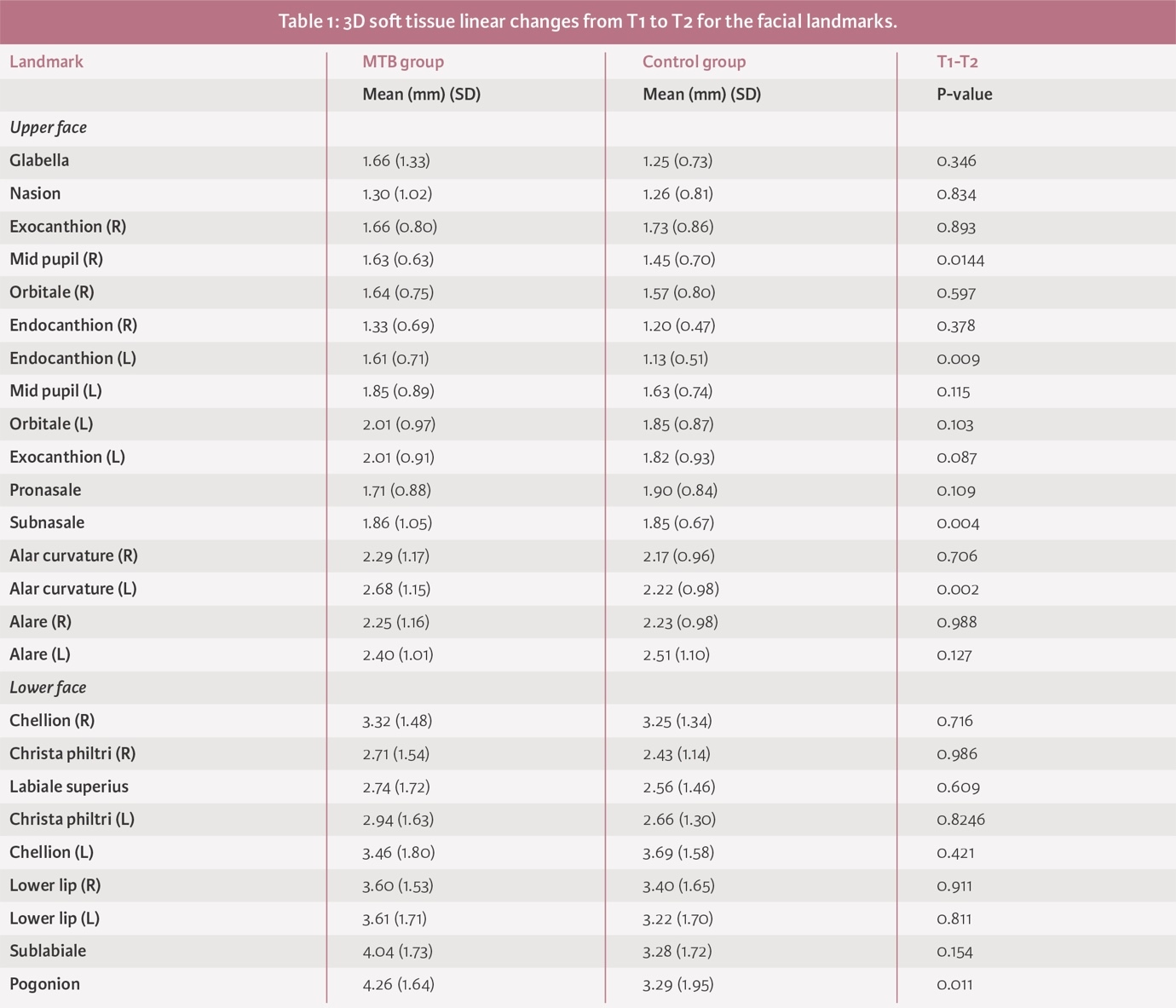
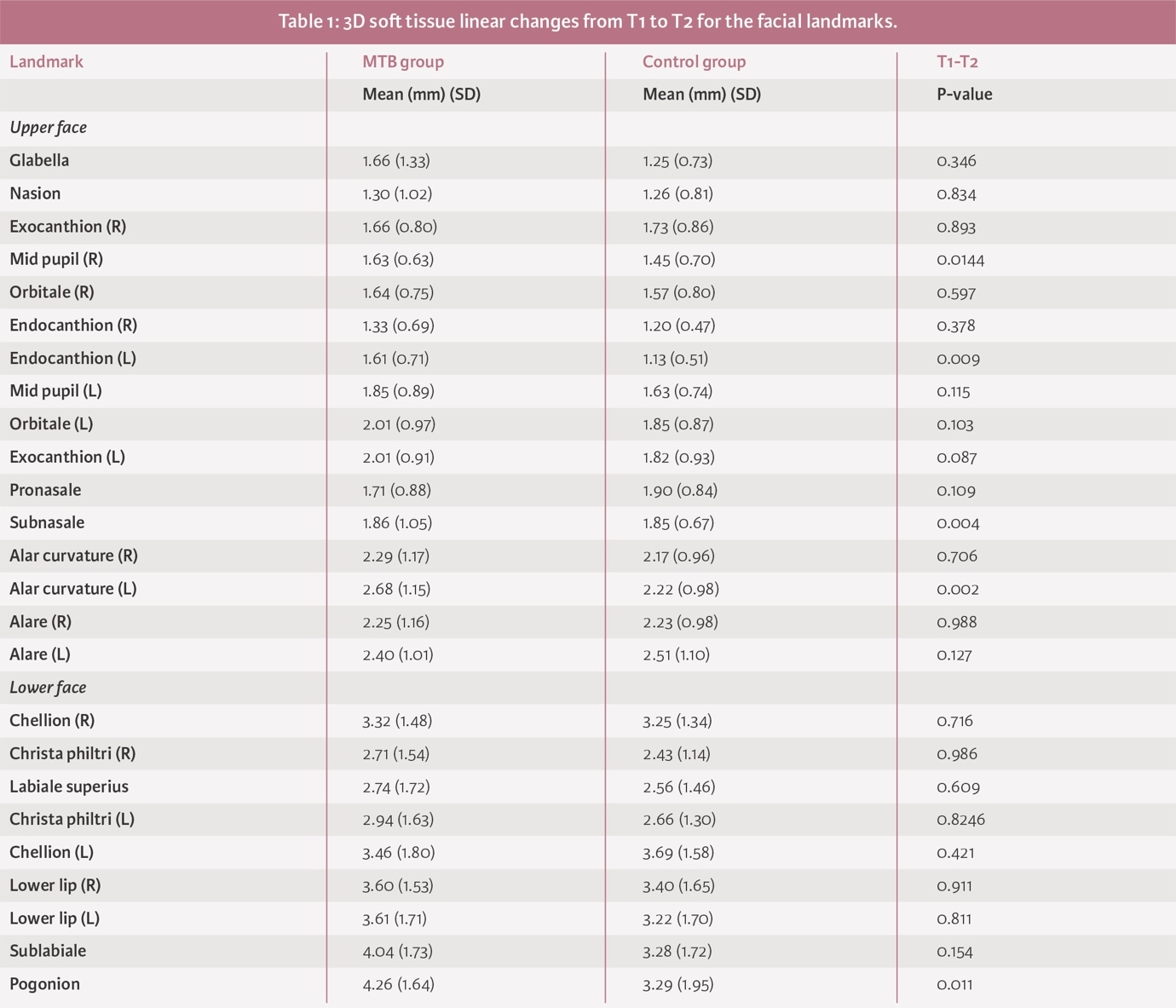
3D soft tissue linear changes in MTB and control groups from T1 to T2
Mean soft tissue linear changes in the lower facial landmarks only differed significantly at the pogonion between treatment and control groups (4.26mm (SD 1.64) and 3.29mm (SD 1.95), respectively; p<0.01) (Appendix 1).
Discussion
This study, undertaken in a State-funded orthodontic service in the RoI, appears to be the first to make a direct comparison of OHRQoL, self-esteem, family QoL, AC-IOTN and 3D soft tissue facial changes between non-randomised samples of those undergoing Phase 1 orthodontic treatment for II/1M and a similarly aged, untreated II/1M group.8,10 This study design has selection bias, and a randomised controlled trial would have been the ‘gold standard’, but was not adopted due to the demands of the waiting list. Regarding the primary outcome measure of OHRQoL, limited evidence exists for children with II/1M before and after MTB treatment compared to those with II/1M awaiting treatment. Previous studies have been cross-sectional, did not have an untreated II/1M control group for comparison, or used a different design of twin block appliance.6,8,12,13
Child-reported outcomes
OHRQoL
Unsurprisingly, participants in both groups had poor OHRQoL at T1, reflecting the negative impact of increased overjet.5
Self-esteem
The absence of a significant difference between or within groups at T1 and T2 likely reflects the complexity of self-esteem as a psychosocial construct, affected by multiple factors. Self-concept, however, has been shown to improve in other studies with Phase 1 functional appliance treatment.5
Child perception of the AC-IOTN
A significant improvement was recorded over time in the MTB group, but this measure remained relatively static in the control group. This is indicative of the positive impact of overjet reduction on aesthetic appearance.
3D changes in lower face
Soft tissue pogonion moved forward significantly in the MTB group. This change, although statistically significant, was modest. A wide variation in growth patterns in II/1 M exists.24
Parent-reported outcomes
Perception of child’s OHRQoL
At T1, the MTB group parents rated their child’s OHRQoL to be significantly poorer than control group parents’ ratings, which may be related to time on a treatment waiting list and anticipation of imminent treatment. At T2, however, a significant improvement was recorded in the MTB group parents’ perception of their child’s overall OHRQoL and across the four domains. In contrast, the control group parents’ perception of their child’s overall OHRQoL did not change significantly from T1 to T2, or across any of the domains. These findings may demonstrate the benefit of Phase 1 treatment for a parent’s perception of their child’s OHRQoL – similar to that recorded in a previous study,5 which employed a different twin block design.
For children in both groups, the parent-reported OHRQoL was poorer than that reported by the child. This is an area for future research, as findings of previous studies have been equivocal.
Family QoL
Phase 1 treatment with an MTB significantly improved family QoL, compared to the control group, demonstrating an impact of treatment beyond the patient.5,25
AC-IOTN
For the MTB group, parental perception of their child’s AC-IOTN improved significantly; however, this perception worsened insignificantly for the control group. Once again, these findings reflect the perceived aesthetic benefit of Phase 1 orthodontic treatment.
Study strengths
There are several strengths to this study, which include the following:
-
a focus on children with II/1M, which is the most referred and treated malocclusion group in the State-funded orthodontic service in the RoI;
-
its prospective longitudinal nature;
-
the recording of child- and parent-reported outcomes; and,
-
the assessment of 3D facial soft tissue changes.
Study shortcomings
These include:
-
a relatively short duration;
-
not adopting a condition-specific measure of OHRQoL in relation to malocclusion (this study, however, aimed to identify the impact on both the child and parent using a comparable instrument);
-
non-randomised samples of severe II/1M, with the associated selection bias;
-
not all subjects in the control group returned for follow-up, due to parent reluctance to attend during the Covid-19 pandemic. Despite this, sample size requirements of 15 males and 15 females in each group were met; and,
-
demographic data were not collected for parent groups, so assessment of the impact of parent gender on responses was not possible.
Conclusions
Phase 1 treatment with an MTB positively impacted child OHRQoL, family QoL, and child and parent perception of AC-IOTN, but did not impact child self-esteem. 3D facial soft tissue changes were modest. Child and parent perception of OHRQoL and AC-IOTN were discordant.