

Learning objectives
After reading this article, readers should be able to:
-
discuss the most common indices used for assessing tooth wear;
-
outline the most frequently used tooth wear indices in clinical practice and hospital settings; and,
-
discuss the advantages and drawbacks of each index.
Introduction
A steady trend of tooth retention has been observed, with evidence suggesting that tooth retention leads to better oral health-related quality of life.1 This is an important finding to bear in mind. According to the Adult Dental Health Survey 2009, over three-quarters (77%) of the dentate patients in the study exhibited some form of tooth wear. It has been found that males present with more tooth wear than females, although there is no clear evidence as to why this occurs.2 Tooth wear is multi-faceted and can be sub-divided further into: abrasion; attrition; and, erosive types of wear (Figure 1). The former two are mechanical, with abrasion resulting from external sources and attrition from internal mechanisms. Erosion arises from either extrinsic, intrinsic, or a combination of acidic sources.3,4 In 2017, tooth wear was defined as pathological as opposed to physiological when it is atypical for the age of the patient, and causes pain or discomfort, functional problems or deterioration of aesthetic appearance, which, if it progresses, may give rise to undesirable complications of increasing complexity.3–5

The high prevalence of tooth wear imposes the need for a succinct method of documenting this problem.6 Many indices have been developed, which mainly rely on visual examination. One of the earliest indices used to measure erosive tooth wear (ETW) was the one developed by Eccles.7 This was originally created to differentiate between industrial and non-industrial erosion due to their differing appearances. The classification looks at the surfaces of teeth and applies a grading to teeth individually, but does not specify the criteria used. Later, Smith and Knight8 developed the Tooth Wear Index (TWI), which was designed to create a system capable of distinguishing between pathological and normal tooth wear. The TWI works by evaluating four surfaces per tooth but does not explain the thresholds for differentiating pathological and normal wear. The Basic Erosive Wear Examination (BEWE)9 is an example that has been validated for use in clinical and epidemiological studies.10–13 This straightforward index assigns a score based on the most severely affected tooth in each sextant, regardless of how many teeth in that sextant exhibit wear. However, it does not consider the extent of wear across other teeth in the same sextant. Notably, the BEWE does not define clear points to distinguish varying degrees of wear. Additionally, the BEWE recommendations advise against restorative intervention until a cumulative score of 14, with the rationale and clinical implications of this threshold not being adequately addressed in the index or literature. Importantly, the BEWE index applies to all forms of tooth wear, not just ETW. The O’Sullivan index14 utilises a three-tiered coding system. Each tooth is systematically coded to provide an outcome for an individual tooth. However, this has only been advocated for use in recording tooth wear in children and adolescents, isolated really to ETW. The Tooth Wear Evaluation System (TWES)4,15,16 was designed to address perceived limitations in existing indices, with the goal of being more comprehensive but less time-consuming than indices like the TWI. The modular format consists of several individual components that guide the clinician through the evaluation process. Unlike the BEWE system, the scores of TWES are recorded independently rather than being summed. However, this process may be seen as time-consuming from a clinician’s perspective.
In clinical settings, it is crucial to document tooth wear as early as possible, helping to address with the patient the aetiology of the tooth wear in their situation. Inadequate monitoring and failure to intervene in cases of tooth wear may eventually lead to extensive full mouth reconstruction and a reorganised approach to occlusion, in order to increase the occlusal vertical dimension5,9,17 The progression of tooth wear is arduous to assess, due to the subjective findings of different operators, coupled with this being a time-consuming process if utilised for each patient. The recording of the extent of tooth wear is an aspect on which it is hard to gain a consensus. Some clinicians record tooth wear with the use of descriptive terms such as ‘moderate’ or ‘severe’, and this may produce difficulties in intra-operator accuracy due to the subjective nature of these terms, which may lead to inaccurate recordings of the tooth wear present. It was also found that clinicians can have a distinct difficulty in differentiating whether dentine is truly exposed in tooth wear, which can lead to difficulties with grading and recording of the tooth wear long term.17 An alternative approach is the use of an index to document the extent of the tooth wear, with particular emphasis on the lesions that extend into dentine, as this may enhance both inter- and intra-operator reliability. The importance of having an index is crucial both to record information in general practice settings and for data collection for long-term studies. It allows precise monitoring with timely initiation of clinical intervention in practice, and facilitates a quantitative reference point when collecting data for research.
The aim of this article is to answer the following questions:
-
Which were the most used tooth wear indices in research and clinical practice between 2017 and 2024?
-
What are the limits of the frequently used indices, particularly in terms of usability, reproducibility, and applicability?
-
Is there any single index that can be advocated for universal adoption in general dental practice?
Materials and methods
Search strategy
A search was carried out using the PUBMED database, ScienceDirect, and Google Scholar. The following criteria were used to search for the most frequently used indices: “(index OR indices OR grade OR grading system OR grading systems OR measurement OR measurements OR recording system OR recording systems OR evaluation system OR evaluation systems) AND (toothwear OR tooth wear OR tooth surface loss OR attritive tooth wear OR abrasive tooth wear OR erosive tooth wear OR attrition OR dental attrition OR erosion OR dental erosion OR abrasion OR dental abrasion)”.
Inclusion criteria
-
Patient-based studies that were conducted in any setting, i.e., hospitals, private dental clinics, and the community.
-
Observational studies and clinical trials only.
-
Tooth wear in adolescents and adults.
-
Articles published in the English language between 2017 and 2024.
-
Use of an index/record system to record tooth wear.
-
No discrimination was made as to the gender of the population base.
These criteria were independently applied by two authors and the results were filtered starting from the title, abstract reading, and full-text reading. The consistency of the filtration process was checked and discussed until reaching a consensus about the final articles to be included in this review.
Results
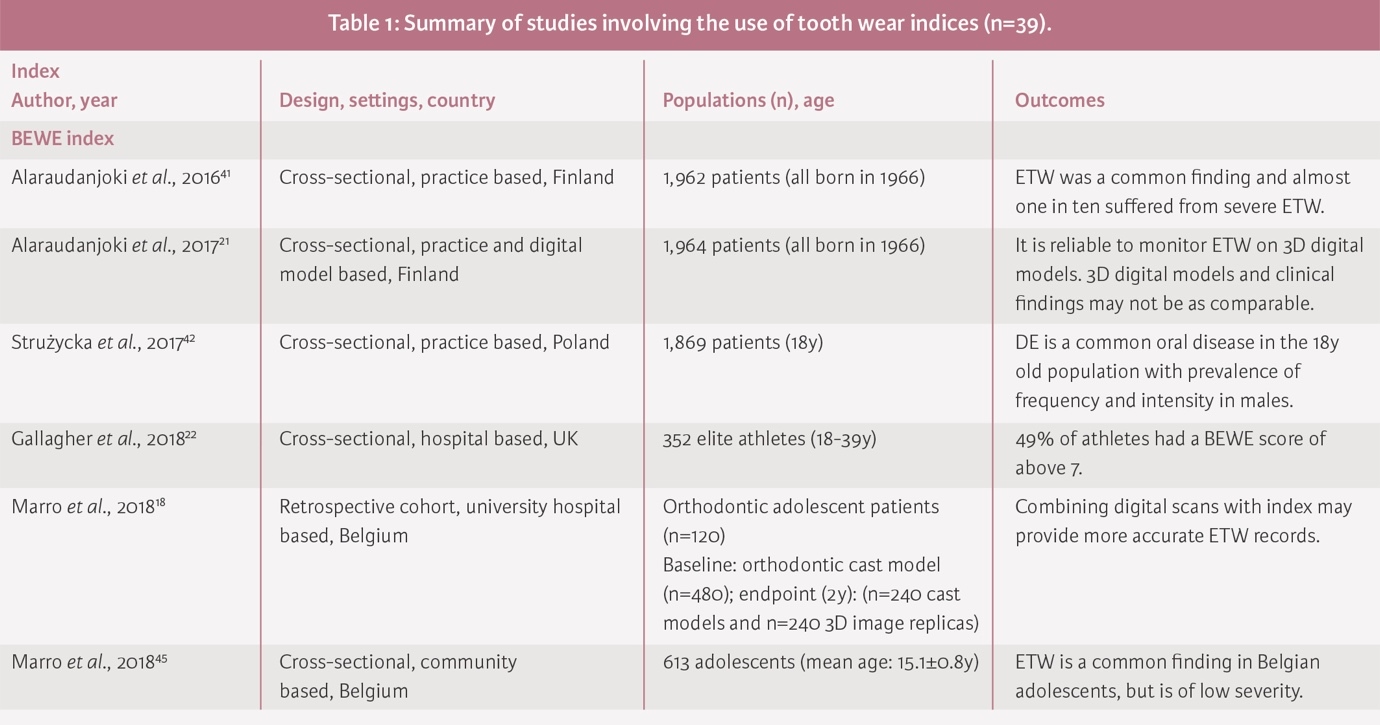
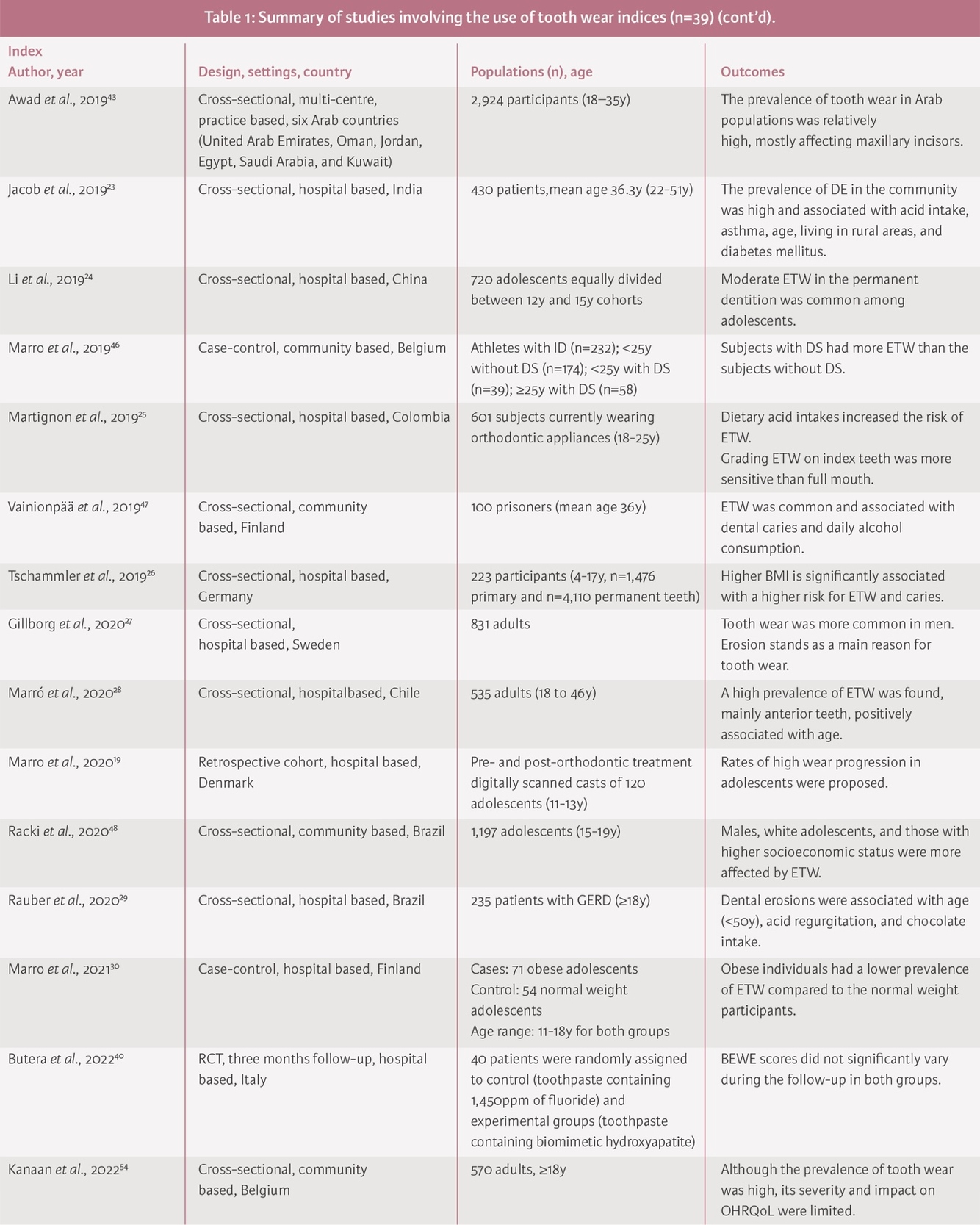
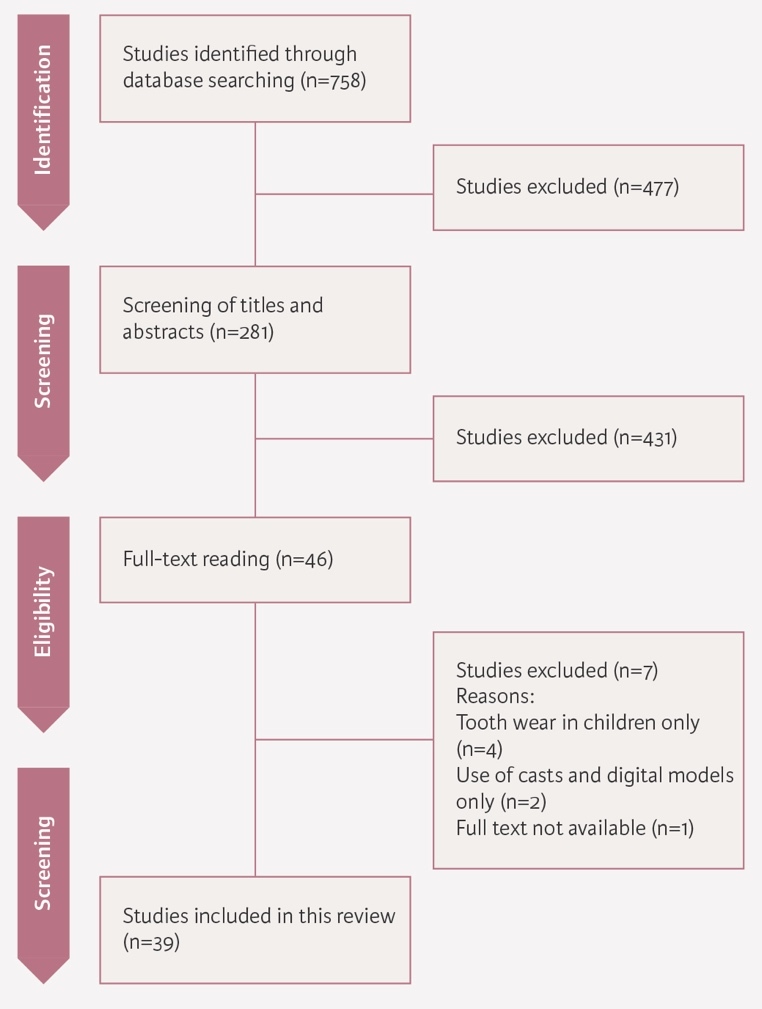
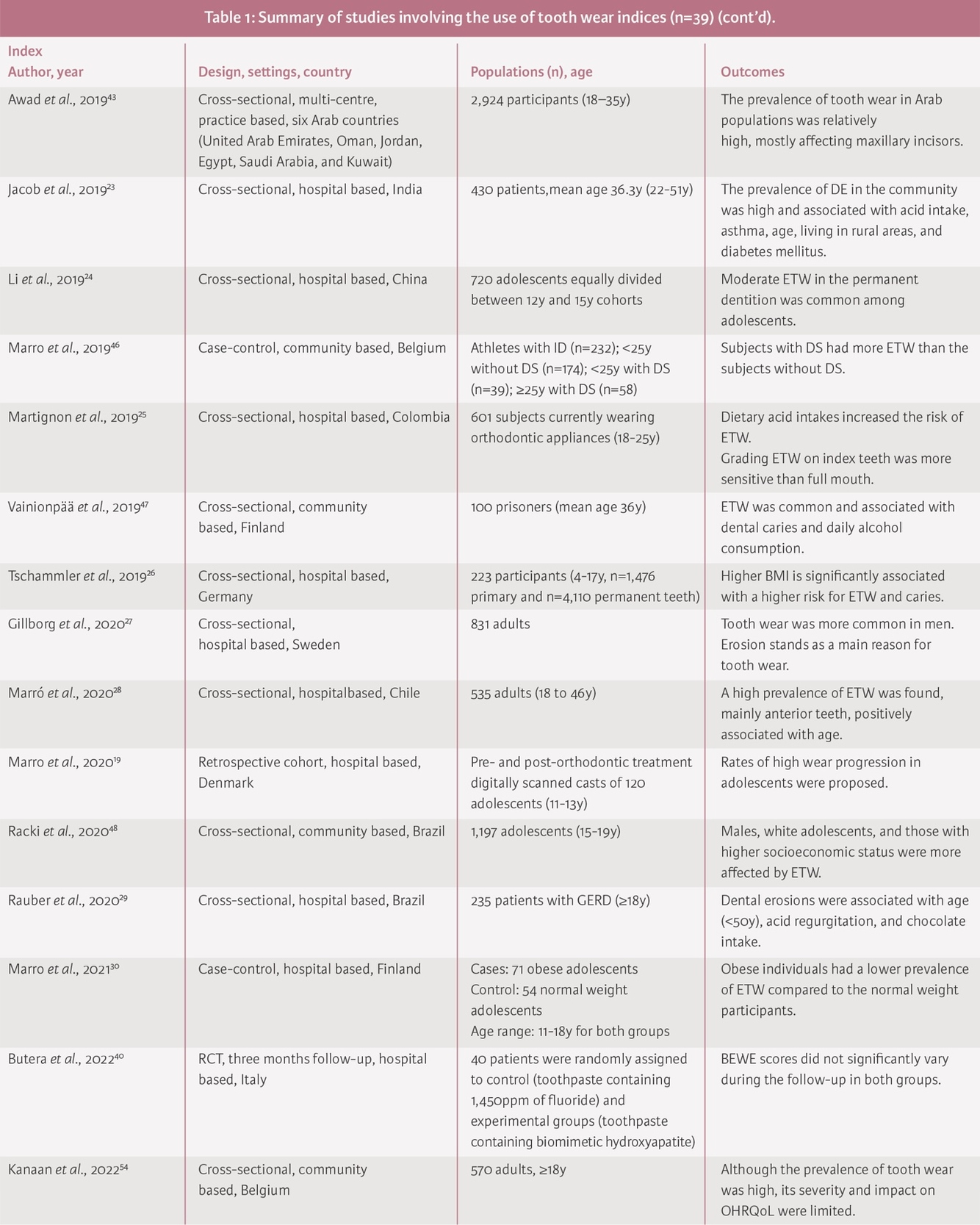
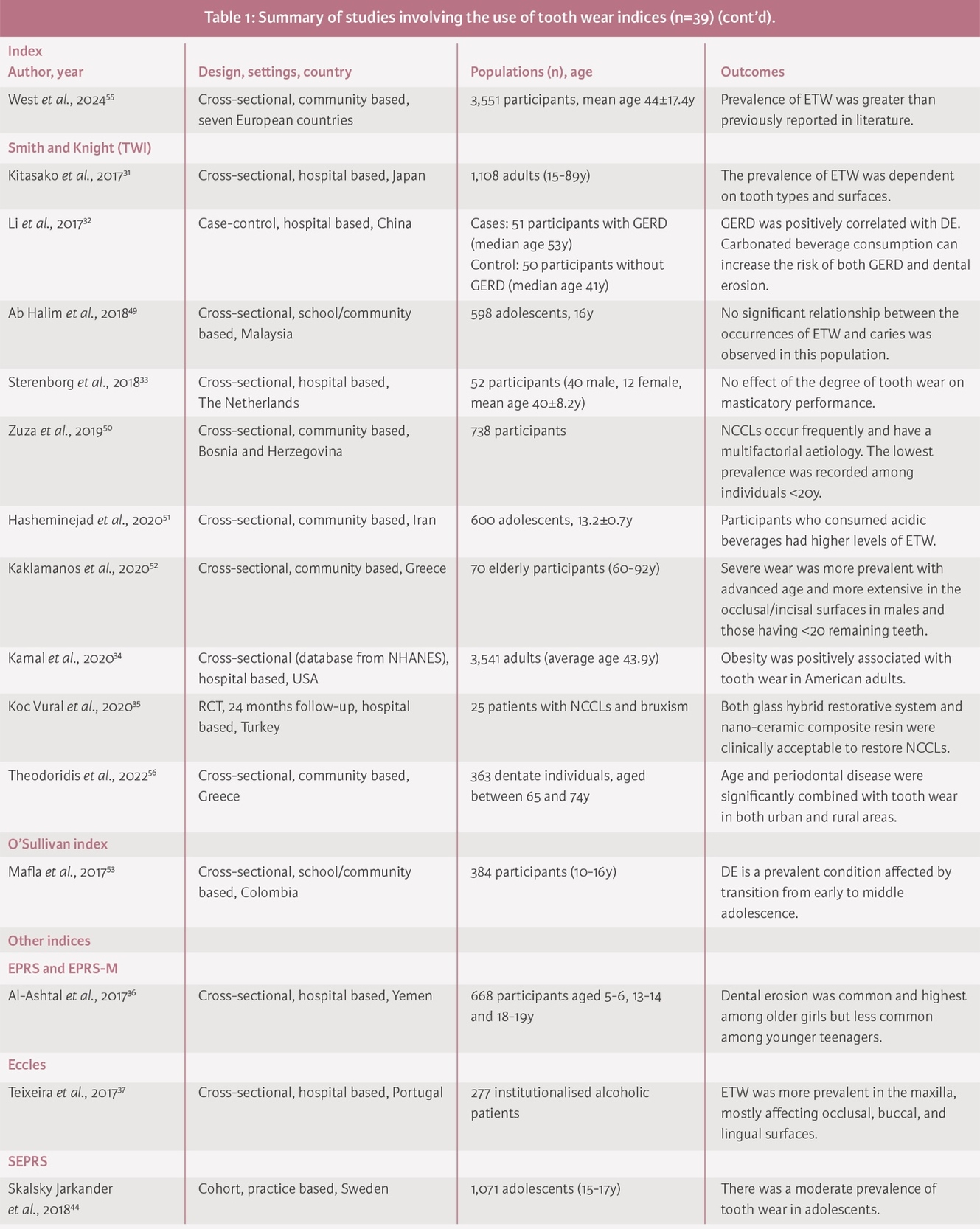
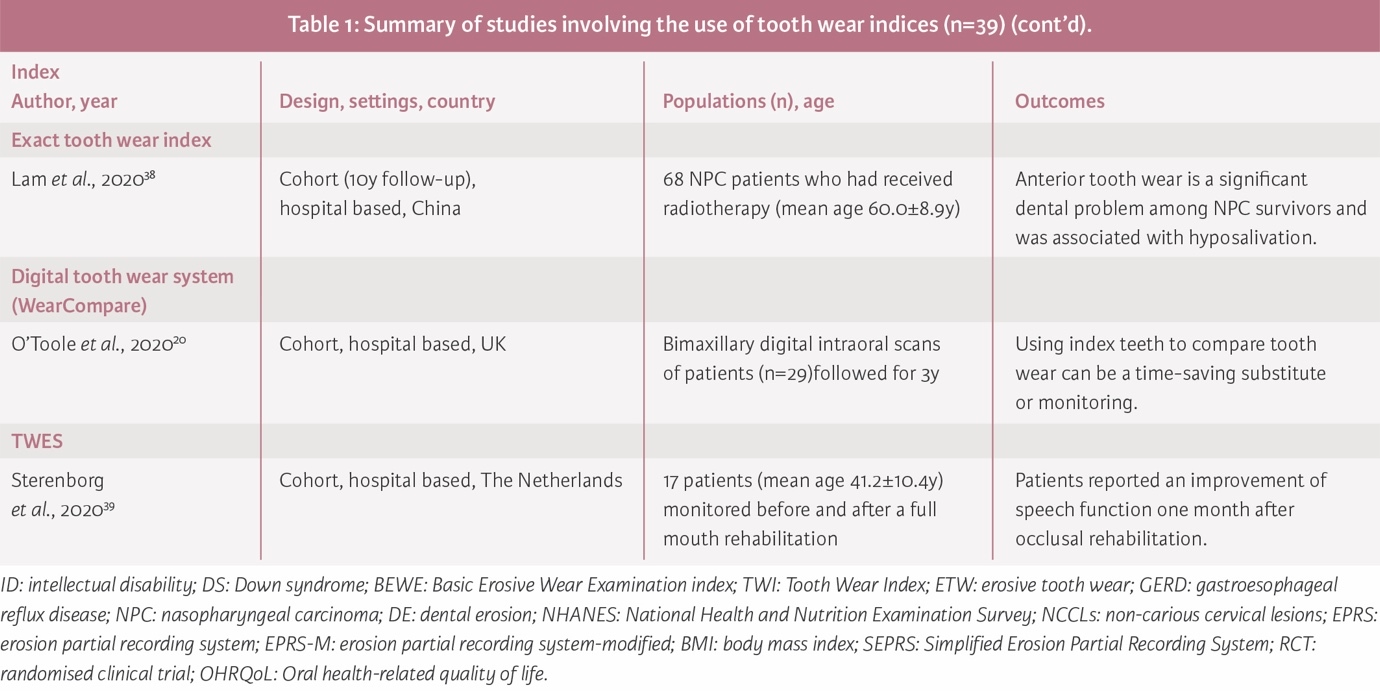
The time was restricted as per the inclusion criteria quoted, which produced 758 results. Of these articles, the relevance of the titles and abstracts was examined to assess which used a grading or index method to record tooth wear. This was followed by full-text reading, reducing the number to 39 articles (Figure 2 and Table 1). These articles ranged from hospital-based, community-based and university settings to studies within a practice setting. Of these, 35 studies were found to have used indices on clinical patients, while four reports combined digital models or dental casts.8–21 Once this was discovered it was then found that most of these articles (n=22, 56.4%) were performed predominantly in hospital settings ^(18-20, 22-40)^ as opposed to general practice (n=5, 12.8%).21–25 The other articles were performed in schools and community settings (n=12, 30.8%),26–37 e.g., care homes and prisons.
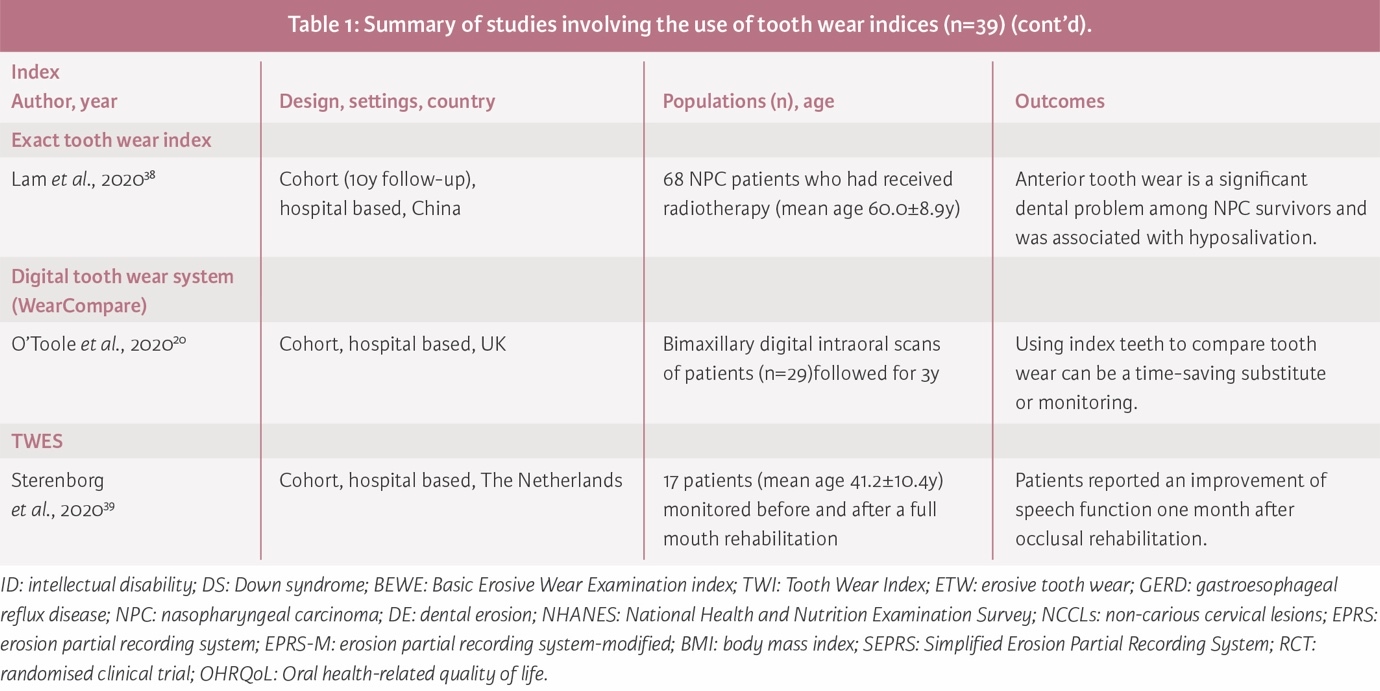
Articles were investigated for the use of any form of index to record tooth wear. Out of the 39 articles that were identified, there was a selection of different indices. These were BEWE, TWI, TWES, O’Sullivan, Eccles, Exact Tooth Wear Index, Erosion Partial Recording System, and Simple Erosion Partial Recording System (SEPRS). Of these indices, the BEWE was found to be the most commonly used18,19,21–24,26–29,35,36,38–47 followed by the TWI,30–33,37,48–52 while other indices were scarcely reported.20,25,34,53–56
Cross-sectional studies were the most common (n=29), followed by cohorts (n=6), case-control (n=3), and only one randomised clinical trial. Most of these studies were conducted in European countries (n=24),18–23,25–28,31,33,35–38,42,43,46,47,50,52,54,56 Asia (n=9),24,30,32,39,40,48,49,53,55 the USA and South America (n=6).29,34,41,44,45,51 The reported prevalence of tooth wear with different severities was relatively high, and increased with age, particularly affecting anterior teeth and males. Additionally, ETW was positively associated with dietary acid intake, alcohol, and carbonated beverage consumption.28,32,39,41,45,49 Some studies suggested that the accuracy of detecting and monitoring tooth wear is improved when combining the indices with digital aids.18,21 Additionally, two studies20,41 favoured using index teeth over full-mouth examination to increase the sensitivity and save time when recording tooth wear.
.jpeg)
Discussion
Although an assortment of tooth wear indices has been developed, none has achieved universal acceptance across research, general or specialist clinical practice. These systems differ in scope, usability and application, with some designed for adults, such as the BEWE, and others, like the O’Sullivan index, more suited to paediatric populations.9,57 Studies on tooth wear would aim to provide insights to drive prevention and treatment. Unfortunately, the intervention seen is often largely dependent on a wider range of systemic factors, including treatment philosophies and policy frameworks.
The universal adoption of a standardised, accepted index remains integral to the global standardisation of data collection, facilitating analysis across varying populations and tailoring treatment in a timely, effective manner.
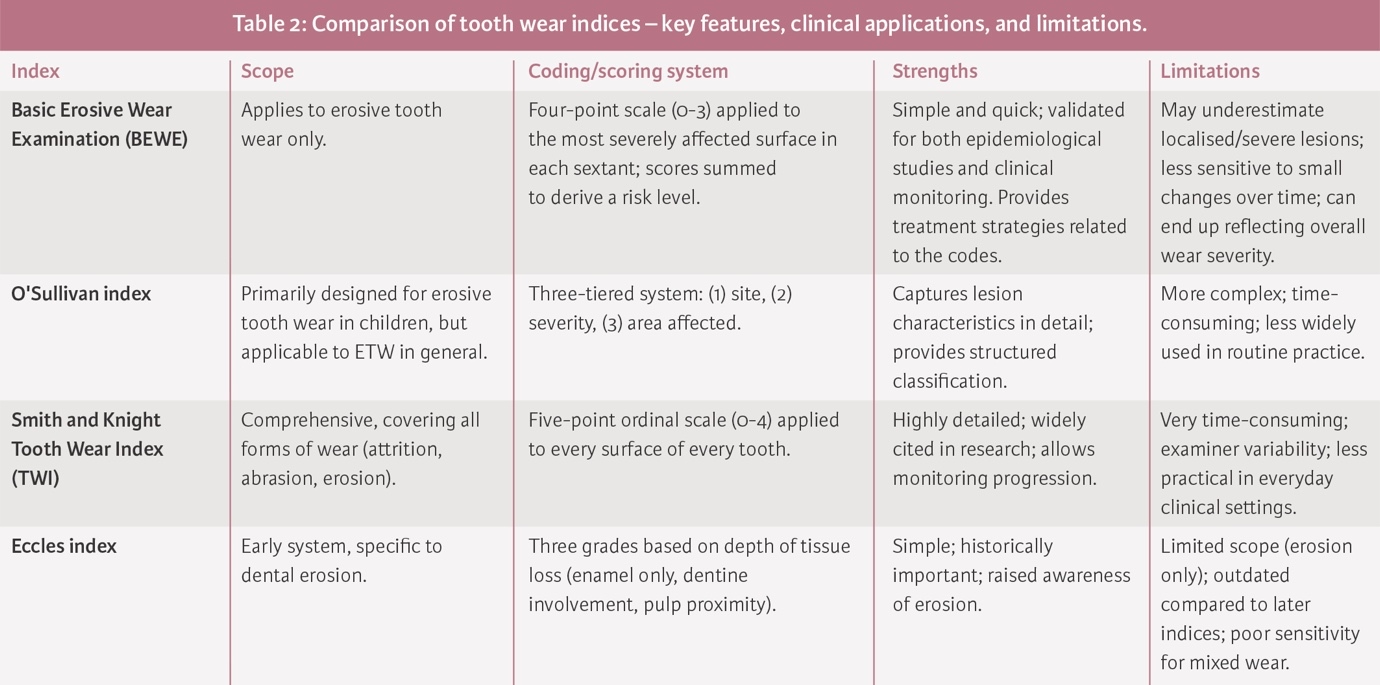
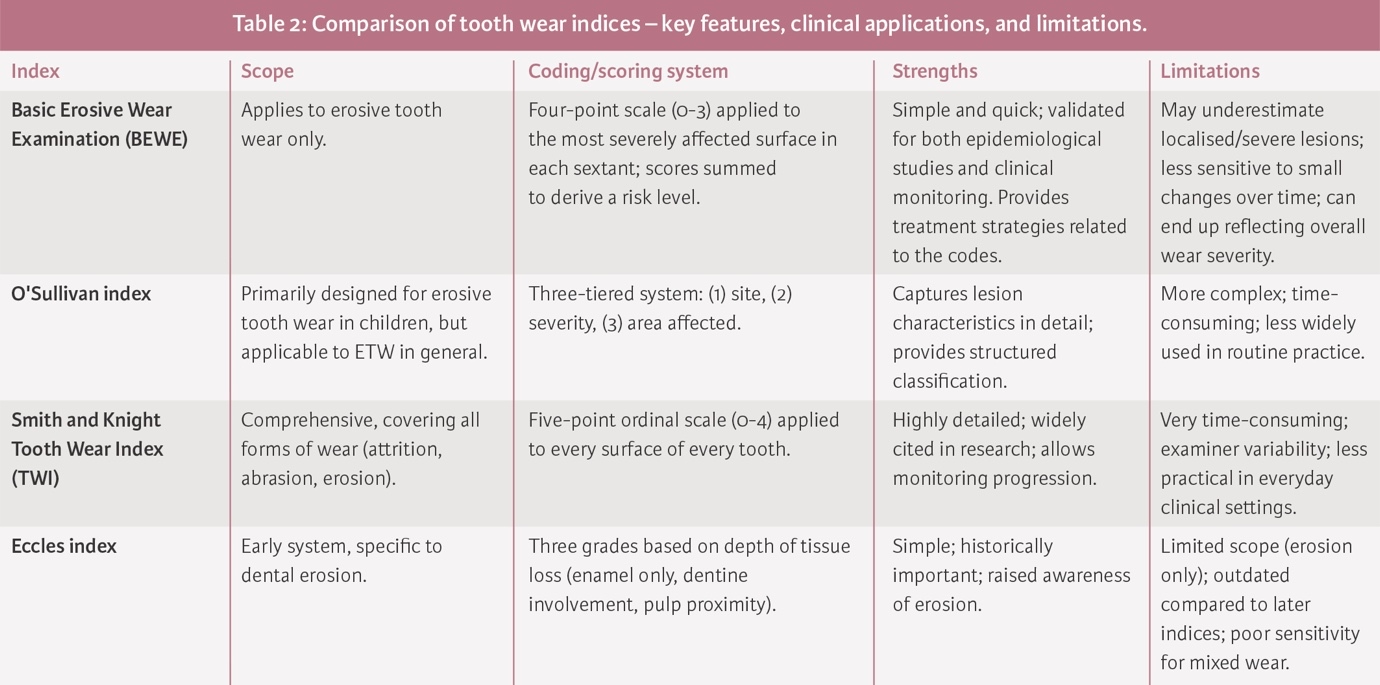
Comparisons of the tooth wear indices
One challenge in comparing the prevalence data from different studies is the variability in the indices used. To better illustrate a comparison between these indices, Table 2 provides a relative overview of their key features, clinical applications and limitations. For instance, one study using the BEWE index alongside the O’Sullivan index highlighted inconsistencies in prevalence reporting, demonstrating how different indices can yield varying results and make inter-study comparisons difficult.34 For the Eccles index, care should be taken as it was created in a hospital setting,7 which meant that the population it was based upon already had severe tooth erosion. Therefore, it was possibly more geared towards the classification of more severe tooth wear and not readily relatable to a general population. Another issue with the Smith and Knight TWI is that surfaces with large restorations are excluded from scoring,8 thereby reducing the total number of surfaces evaluated. However, while the index has been used as a reference for assessing wear across age groups, the basis is hypothetical and relies on speculative observations.
These variations are further compounded by factors such as cultural differences and the sample sizes of the studies, which can either overestimate or underestimate the true prevalence of tooth wear. Without a standardised approach to indexing and training among clinicians, it remains challenging to accurately compare data across different populations and studies.26,58
The indices examined in this article utilise a quantitative scale for the grading of tooth wear. These range from simple indices, such as the Eccles index, to more multifarious ones like TWES index. The Eccles index was designed to document erosion caused by non-industrial factors.7 However, it primarily focuses on ETW and does not account for the other modalities of wear, potentially limiting the scope of its clinical usefulness. As Smith and Knight have noted, tooth wear often results from a “combined cause”, making it difficult to rely solely on a single aetiology for measurement.8 On the other hand, the complexity of the TWES and the TWI make their application laborious, especially during first visit examinations in a general practice setting. In contrast, indices like BEWE and Eccles are more appealing due to their simpler scoring systems. However, a shortcoming of this simplicity is that it may result in the omission of critical data about individual tooth surfaces, making it harder to monitor the progression of tooth wear over time. The O’Sullivan index, specifically designed for children and adolescents, positions itself as a well-structured exemplary model for recording tooth erosion in younger populations. Its focus on the extent of tooth surface loss is particularly relevant. Other indices may use the presence of secondary dentine as a key factor in assessing tooth wear, but this feature is less applicable in younger patients, making the O’Sullivan index more apt for this wide demographic of patients.14
Monitoring tooth wear
Tooth wear results from the irreversible loss of dental hard tissue, emphasising the importance of early monitoring and precise documentation. Accordingly, the guidance from the Royal College of Surgeons (RCS) England encourages maintaining good tooth wear records; however, restraint is advised regarding the use of these indices. This caution largely arises from concerns about index reproducibility, both between clinicians and among individual clinicians over time. It is advised that alongside indices, accompanying methods such as clinical photographs and putty indexes should be used to create a more comprehensive record of tooth wear progression.
The limitation of relying solely on indices for monitoring is that many were originally designed to aid in treatment planning rather than tracking the progression and severity of wear. It appears that the indices may not be fit for purpose. These indices tend to emphasise dentine exposure rather than enamel loss, leading to higher severity grades. Among the indices, only the TWES explicitly mentions its applicability in monitoring tooth wear over time, while the others are more suited for diagnosis and epidemiological studies.
In the era of intra-oral scanners, these now provide a valuable tool for the recording of tooth wear, with the ability to superimpose and compare data over varying time periods.59 While the use of photographs provides a valuable means of documenting tooth wear, its practicality in routine general practice may be limited, and it requires high-quality images taken with a digital single-lens reflex (DSL-R) camera. The BEWE index is frequently favoured due to its structural similarity to the universally used Basic Periodontal Examination (BPE) index, making it simpler for clinicians to adopt and translate to daily use. However, the BEWE’s tendency to group teeth within a sextant under a single score can lead to inaccurate assessments, potentially exaggerating wear severity.60
Calibration and inter-examiner similarities
One noteworthy challenge associated with the use of an assorted selection of indices is the difficulty in maintaining inter-examiner reliability. Most studies require clinicians to undergo calibration and acquire experience before employing any specific index.61 However, after initial calibration, the risk of examiners becoming de-calibrated over time exists, reducing recorded data accuracy. This examiner record discrepancy is a known problem inherent to all grading systems.62 For example, one study investigating the use of indices by general practitioners in England found minimal inter-examiner agreement when using the BEWE index, with a Fleiss’ Kappa score of 0.12, where a value between 0.81 and 1.00 is considered to reflect perfect agreement.63,64 In contrast, the O’Sullivan index has been reported to have a reproducibility rate of 70-93%, comparable to the 79.5% reproducibility observed in a study by Smith and Knight.8,14 Notably, this did not include a cohort of general dental practitioners.
It is accepted, ultimately, that every index requires a degree of learning, practice and familiarity before examiners can produce consistently reliable results that can be meaningfully translated.
Conclusions
There is currently no universally accepted and ideal index that meticulously captures all aspects of tooth wear diagnosis, in an easily reproducible and useful format. This review revealed a wide range of indices available for recording and diagnosing tooth wear. Subjectivity and lack of quantifying loss of tooth structure is a shared drawback among all indices that compromise the sensitivity and specificity of indices.
There exists a healthy research interest in tooth wear, and numerous indices remain in active use by researchers. However, the majority of these studies were conducted in industrialised and developed countries, pointing to a global lack of awareness about tooth wear as a major oral health problem. There needs to be a well-defined, future-focused research theme, geared to developing a universal index, that can be translated between researchers and the general dental practitioner. However, as with other indices, simply recording a score should not mark the finale of clinical responsibility. Treatment decisions are multidimensional, considering not only the score, but age, social factors, and risk factors. The high variability in indices underscores varying treatment philosophies.
No index can be regarded as truly ideal, particularly given that most patients are first managed in primary care. This setting is uniquely influenced by time constraints, resource limitations and patient variability. If taken collectively, these challenges underpin the importance of developing a universally accepted index, one that balances reliability and practicality across both the research and general practice settings.