






Introduction
Ectodermal dysplasia (ED) is a hereditary disorder1 that is caused by dysplasia of one or more of the ectodermal tissues and their accessory structures.2 The disorders are congenital, non-progressive and diffuse, with a worldwide prevalence of approximately seven per 10,000 births.3 The primarily affected tissues include hair, skin, eccrine glands, teeth and nails.
The two most common syndromes of ED may be broken down into hidrotic ED and anhidrotic ED (hypohidrotic ED).1 The more common phenotype is anhidrotic ED and is a rare X-linked condition. It is also known as Christ-Siemens-Touraine syndrome and is characterised by several defects including onychodysplasia, hypohidrosis, hypotrichosis, and an atypical dentition.4
Males affected with ED may present with hypotrichosis, hypodontia or anodontia, and without eccrine sweat glands. In females, eccrine sweat glands may or may not be present.5
The most common oral characteristic in many cases of anhidrotic ED is hypodontia or anodontia6 with Yenisey, Guler and Onal (2004)7 stating that prosthetic rehabilitation is a routine process for patients with ED. Literature comparing hypodontia between males and females found that almost all males had hypodontia, whereas hypodontia was present in 73% of females, and with great variability in terms of severity and presentation.8 However, Rosa et al. (2012)9 found that there were no statistically significant differences in hypodontia of one or more types of teeth between genders in patients with ED.
Some people with ED may also present with prominent supraorbital ridges, sunken cheeks, frontal bossing, everted/thick lips, a saddle nose, hypoplastic alae nasi, large, low-set ears, and hyperpigmented skin.1 Other common symptoms include an absence of mucus glands in the oesophagus, duodenum, upper respiratory tract and bronchi, eye abnormalities including photophobia and decreased tearing, and a shortened stature.10
From a dental perspective, both the deciduous and permanent dentition are affected. Common dental concerns in patients with ED include conical or peg-shaped teeth (predominantly in the anterior dentition), hypodontia or anodontia, hypoplastic and atrophic maxillae, hypoplastic teeth, and a delayed eruption of the permanent dentition.11
Extensive dental intervention is needed from early childhood onwards to manage the absence of deciduous and permanent dentition, with a multidisciplinary team (MDT) approach recommended to ensure the best outcome for patients affected by ED.12 Several authors have reported osseo-integrated implants as a prosthodontic treatment option for adults with anhidrotic ED.6
This case report outlines the positive application of the MDT approach in the successful management of an adult female patient with ED, a hypoplastic maxilla and hypodontia. It highlights the appreciation of sound diagnostic principles and treatment approaches in comprehensively addressing patient concerns. It hopes to highlight to dental professionals the clinical skills required, the benefit of piezoelectric systems in performing oral and maxillofacial surgery (OMFS) in patients with ED, and the crucial importance of interdisciplinary care when treating patients with ED.
Materials and methods
A 36-year-old female patient presented to the Restorative Department in Dundee Dental Hospital and Research School with concerns relating to her facial appearance and problems with an existing upper denture leading to social embarrassment. Medically the patient had anhidrotic ED, an associated lack of development of secondary dentition, and velopharyngeal incompetence. She had previously been considered for orthognathic surgery four years prior, but due to the significant risks to velopharyngeal function and a lack of available evidence associated with a LeFort 1 advancement at that time, it had been deemed inappropriate.
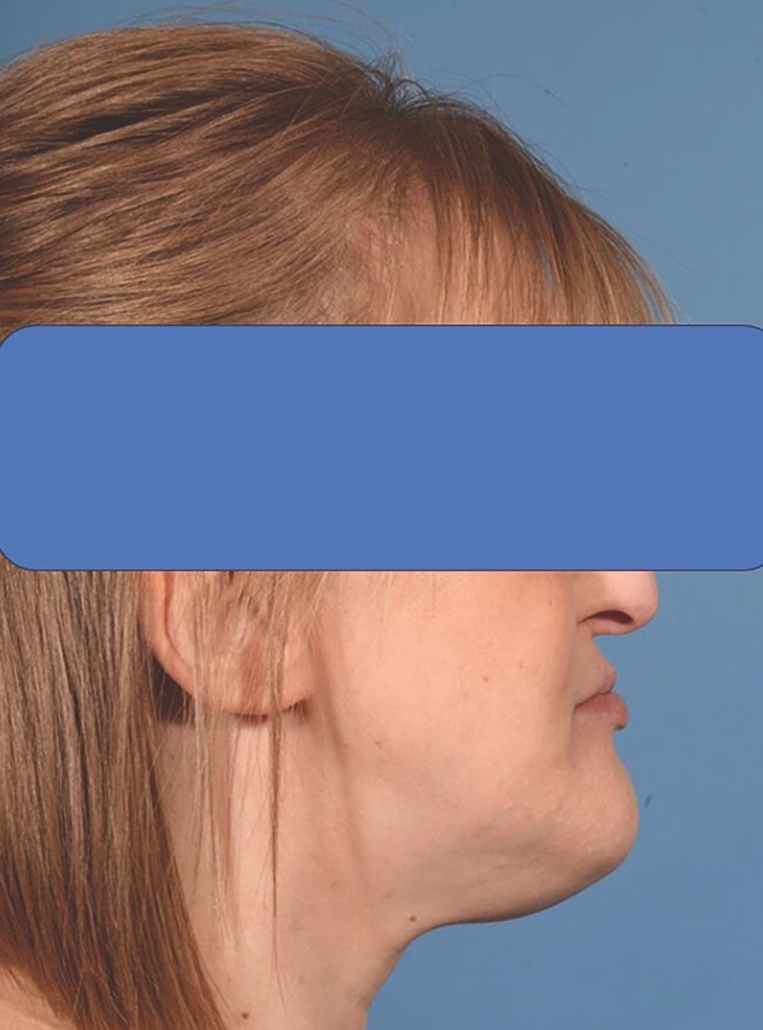
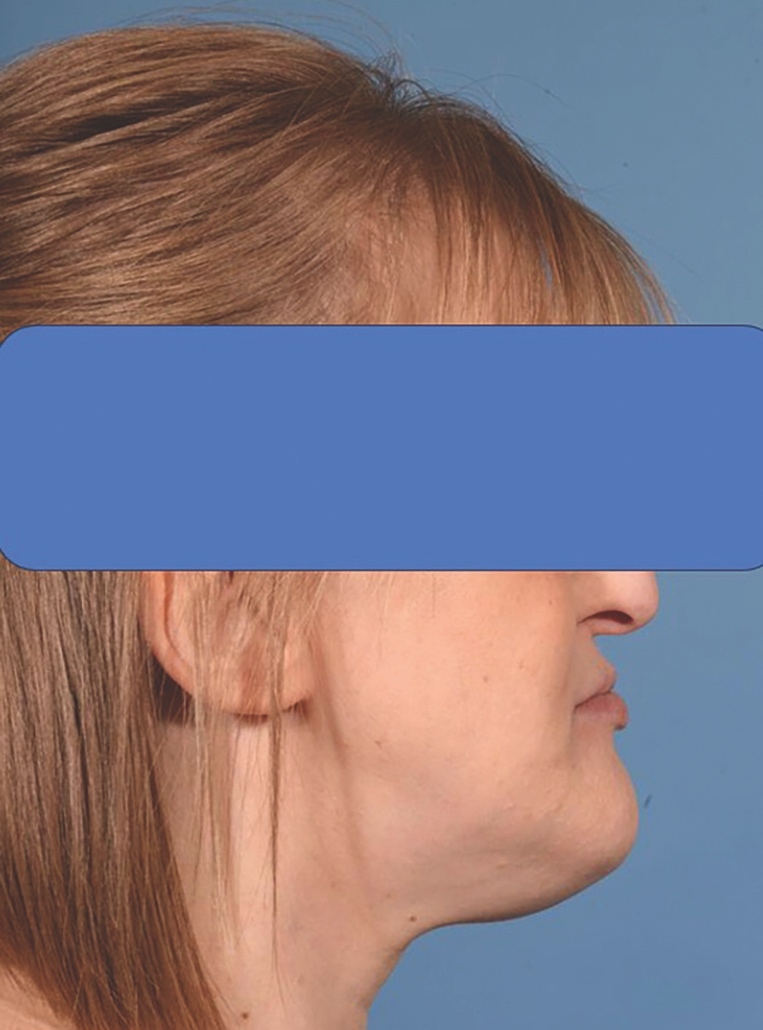
Upon clinical examination, she presented with a Class III skeletal pattern (Figure 1) with average vertical proportions, a hypoplastic maxilla, and she was edentate. She had undergone multiple previous attempts at denture construction; however, these were of limited success.
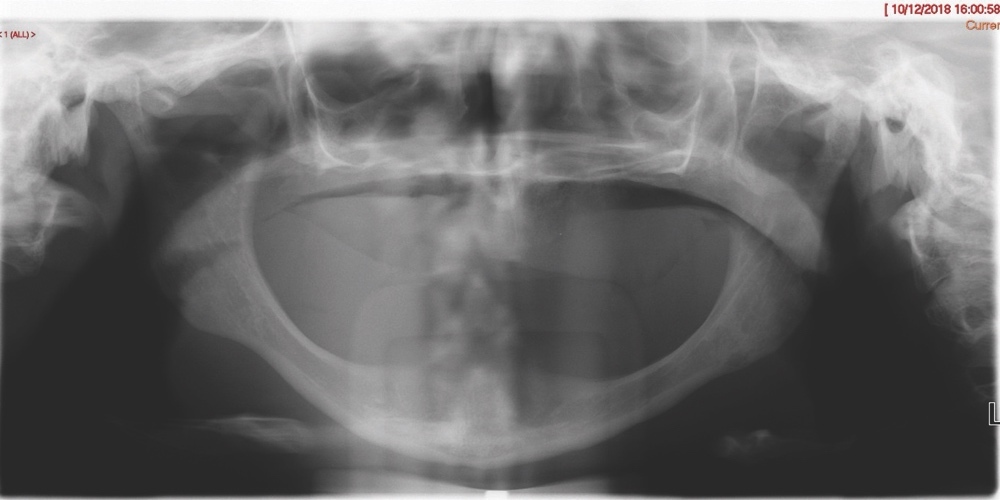
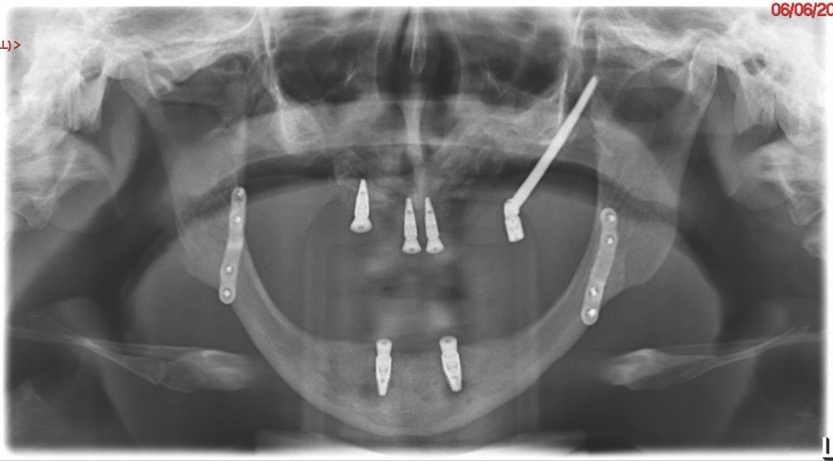
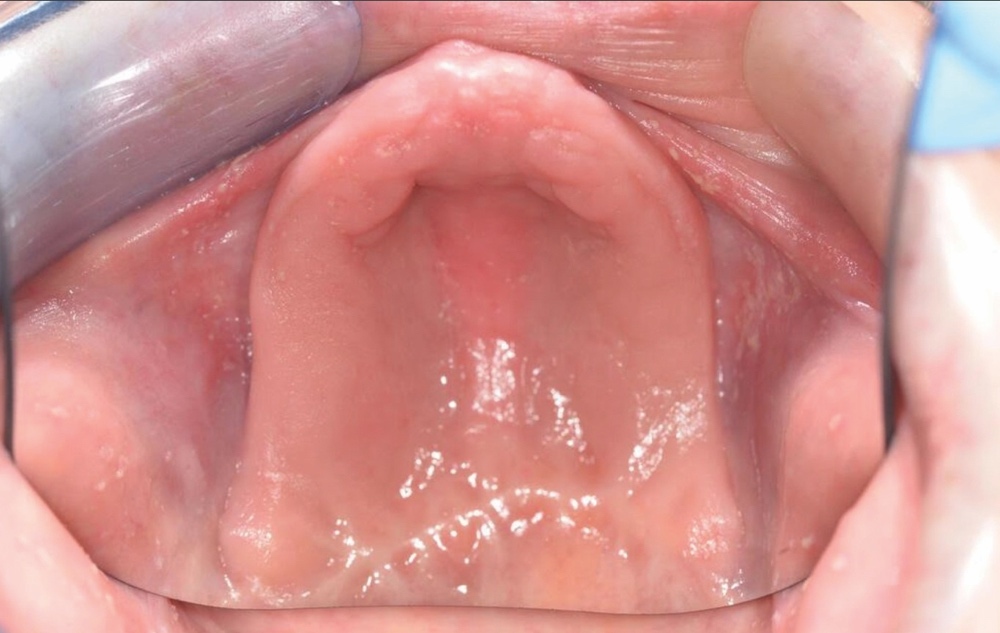
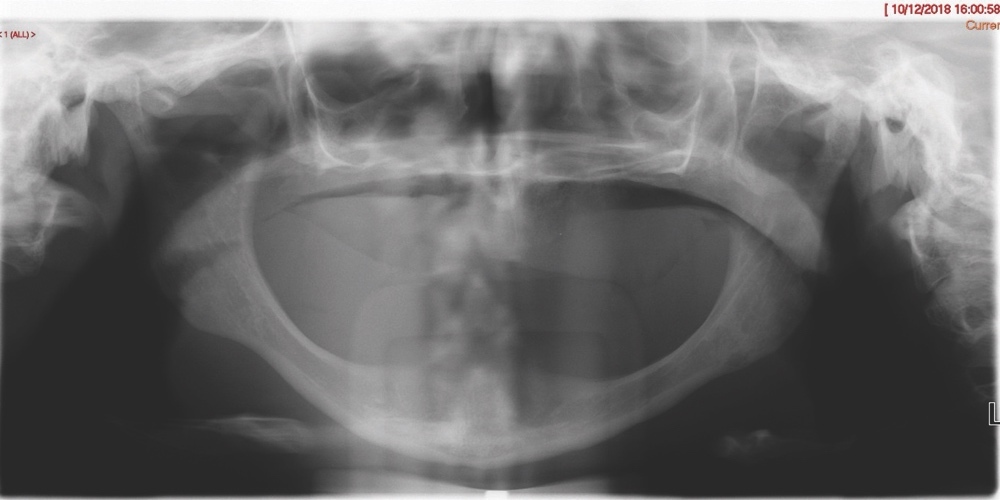
Intra-orally, the patient presented with an atrophic mandible and maxilla (Cawood and Howell13 Class VI and V, respectively) and was edentate (Figures 2 and 3). An orthopantomogram (Figure 4) confirmed the clinical findings and also demonstrated the proximity of the reduced maxillary ridge height to the maxillary sinuses.

Following clinical and radiographic findings, it was deemed that an MDT approach was required to comprehensively manage the patient’s skeletal and dental concerns, and she was referred to the OMFS Department, where she was jointly assessed by a consultant in OMFS, a consultant in orthodontics and a consultant in restorative dentistry. Using multiple 3D printed models in an OMFS laboratory, cone beam computed tomography (CBCT) imaging, 3D planning software (KLS Martin Group) and Straumann’s coDiagnostiX dental implant planning software, an OMFS consultant and a consultant in restorative dentistry planned the positioning of the implants on the 3D printed models. A consultant in orthodontics provided input to the planning of the skeletal movements in relation to the overall positioning and relationships of the dental bases for subsequent restorative treatment. They also provided input to the inclinations of the dental implants and subsequent denture teeth in association with the OMFS surgeon and restorative dentist throughout treatment. The three consultants decided upon the use of the piezoelectric system as part of the OMFS, to ensure that the optimal patient outcome was achieved.
Treatment options were discussed with the patient and it was agreed to pursue the following treatment plan:
-
Two-step surgical approach including:
a) bimaxillary osteotomy and bone grafting; followed by,
b) delayed insertion of transzygomatic and conventional dental implants (once adequate OMFS healing and successful bone grafting was confirmed). -
Restorative dental treatment to include a full arch maxillary bridge and a lower implant-retained and -supported denture (once adequate healing of implants was confirmed).
This staged sequence was carefully chosen by the MDT during pre-operative planning to ensure maximum implant stability and long-term success, and was based on sound clinical and biological principles to optimise bony healing and graft integration prior to implant insertion. The aims of treatment were:
-
To improve the patient’s skeletal and soft tissue profiles.
-
To address the insufficient alveolar height and width, sulcus depth and incisal show of restorations.
First step of surgical approach: orthognathic surgery with bone grafting
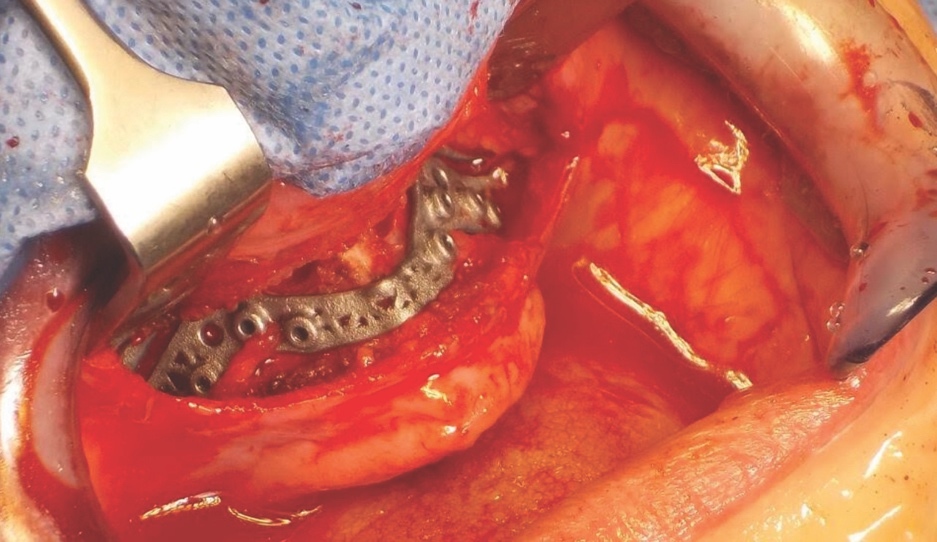
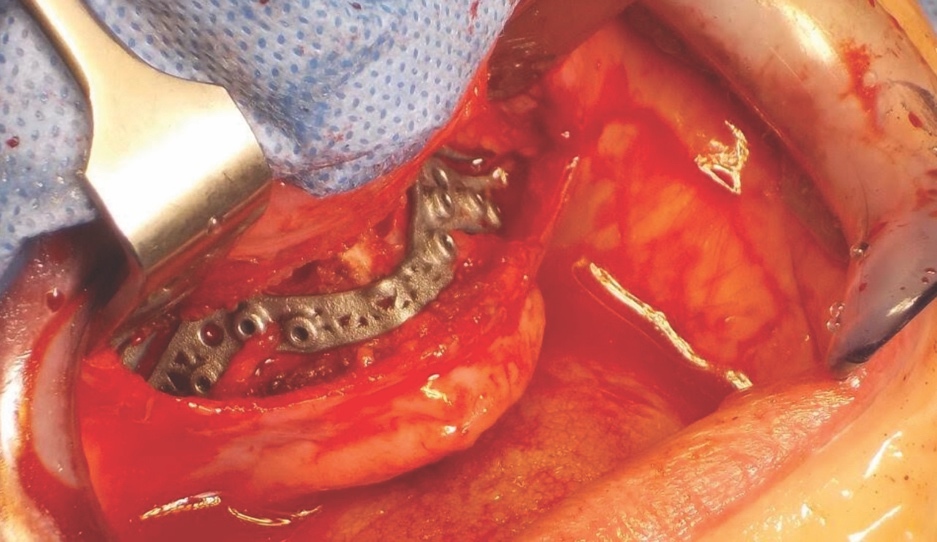
Following careful informed consent, the patient was treated in the OMFS Department in Ninewells Hospital. The first surgical stage was completed with a bimaxillary osteotomy with 3D guides and plates (KLS Martin) followed by bone grafts from the left iliac crest to the maxilla and mandible (Figure 5). The maxilla was advanced 10mm and set down 7mm.
Second step of surgical approach: implant placement
Six months after the first surgical procedure, a CBCT scan was taken in order to assess the position of the mandible to the maxilla and MDT discussions were repeated. Radiographic evaluation revealed appropriate healing with stable bone height. The patient then underwent the second stage of her surgical management, and transzygomatic implants (maxilla) and conventional dental implants (mandible) were inserted.
The piezoelectric system was very important in the management of this patient. It was used to split the maxillary and mandibular ridges (UR4, UR1, LL3 and LR2 regions) and also to remove the bone and open the alveolar ridge anteriorly and posteriorly on the right side of the maxilla.
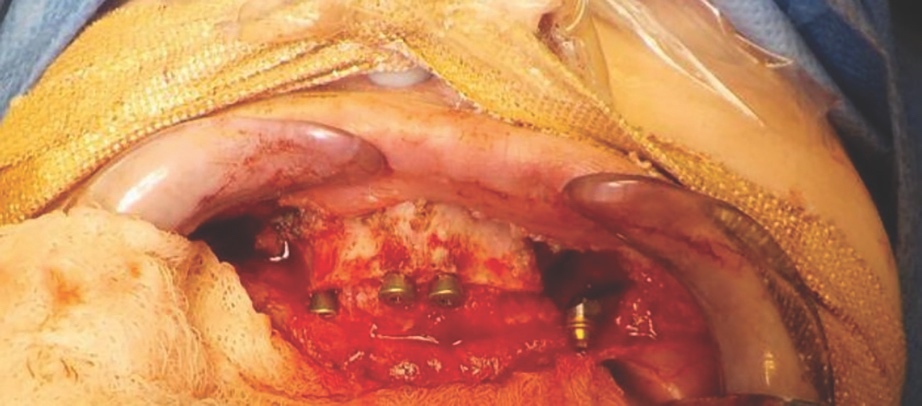
Bone level fixtures were placed in the intraforaminal region with submerged healing, and axially loaded. After alveolar ridge height reduction to facilitate implant placement in the apico-coronal position, one Southern zygomatic implant (Zygex with uniabutment and healing cap) was placed in the left quadrant and three 10mm bone-level implants (021.3310) were placed (UR4, UR1 and UL1 sites) (Figure 6). Two 12mm implants (021.5310)) were then placed in the mandible (LL3, LR2 regions).

Restorative treatment
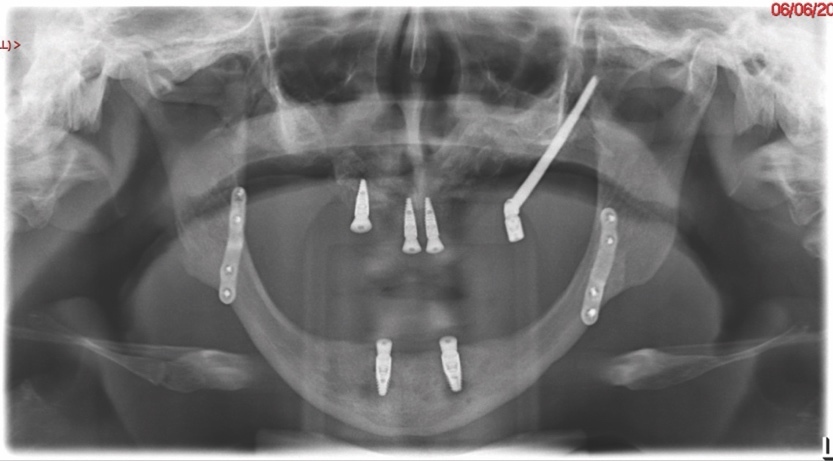
A follow-up orthopantomogram revealed that all implants were healing well (Figure 7). The shortened dental arch (SDA) concept was used to restore this patient’s occlusion, and a maxillary bridge and mandibular implant-retained denture were used to restore second premolar to second premolar in each arch (Figures 8 and 9). SDA was introduced in 198114 and is a problem-oriented method that aims to minimise complex restorative treatments.14 It outlines maintaining at least four posterior occlusal units or a minimum of 20 well-distributed teeth to ensure a functional, natural and healthy dentition.15


Follow-up
Follow-up clinical examination performed 24 months post treatment has revealed a clinically stable and functional occlusion, with minimal relapse post orthognathic surgery and an enhanced facial profile. The patient is very satisfied with the aesthetic and functional outcome, and her skeletal and dental concerns have been successfully addressed.
Discussion
Oral and maxillofacial surgery and the piezoelectric system
The piezoelectric system is a conservative and precise ultrasonic surgical system, which is used to perform orthognathic surgery and designed to be active on mineralised tissues only. It consists of a handpiece and various tips for cutting bone, bone substitutes and teeth. It has a narrow kerf for enhanced precision to perform bone surgery procedures and to reduce the risk to soft tissues.
This device maintains blood-free operation sites through a cavitation effect and allows for precise cutting of the bone by using micro-vibrations at frequencies of 24-29kHz with 60-200µm amplitude to cut through the bone.16 It has been suggested that in comparison to the traditional saw technique used in orthognathic surgery, the piezoelectric device has demonstrated more favourable outcomes in terms of neurosensory disturbance and operative blood loss, and is less traumatic and more efficient.17 The piezoelectric device is used in dentistry in maxillofacial osteotomy, dental implantology, alveolar decortications, resection of cyst and tumour-like lesions, corticotomy and temporomandibular joint (TMJ) ankylosis.18
The novelty lies not solely in the tool, but in the context-specific application, the piezoelectric instrumentation in the osteotomy of an underdeveloped maxilla, which remains under-reported in the literature. This approach allowed cuts to be within a controlled small width and avoided unnecessary bone loss. It also minimised the risk of soft tissue injury. It was initially virtually planned that the patient would have one zygomatic implant placed on each side; however, unfortunately, due to limited zygomatic bone volume, it was felt intra-operatively that this was not appropriate. Instead, a ridge split was performed to allow placement of dental implants into the maxilla. Using the piezoelectric saw allowed for widening of the mandibular alveolar ridge without the risks associated with chisels and osteotomes. The precision and safety profile of piezoelectric instruments made it the essential tool in this situation, as its use was necessitated by the patient’s exceptionally thin maxillary bone. Conventional drills or chisels posed a significant risk of iatrogenic fracture or collateral damage to adjacent soft tissue structures and were therefore unsuitable in this case.
This case outlines the successful application of the piezoelectric system in managing a patient with ED and a hypoplastic maxilla with limited postoperative complications and in achieving an aesthetically pleasing Class I skeletal profile (Figure 10).

Bone augmentation
Previously, patients with ED have had oral function restored with partial or complete removable prostheses supported by teeth or tissue. In recent years, dental implant-supported prostheses have provided an alternative method of restoring form and function to these patients.19
As ED is a genetic disorder associated with premature tooth loss and severe oligodontia, the oral rehabilitation of these patients to improve quality of life and social confidence is of utmost importance.20 The demand for the prostheses to restore aesthetics and function while being comfortable for the patient is paramount. Fixed, implant-supported prostheses have been used to successfully restore some of the complex oral functions in patients with ED.21 However, the quantity and quality of alveolar bone greatly affect the success of implant restorations in these patients.20
As it is common for patients with ED to have hypodontia and thus a reduced quantity of bone, bone grafting procedures are often required prior to implant placement. There are limited reports of successful reconstruction of both the mandible and maxilla with implants in patients with ED.22
In this case, both alveolar bone height and width were lacking as a result of hypodontia. The surgery was undertaken in two separate stages to allow for adequate bony healing post bone grafting, and an accurate assessment of the relationship of dental bases to one another post orthognathic surgery. This was to ensure that a stable result would be achieved with restorative treatment and to reduce the risk of implant malpositioning. A CBCT scan allowed for the identification of alveolar ridge morphology and bone quality, and confirmed the success of dental implants prior to restorative treatment.
3D computer-aided planning system
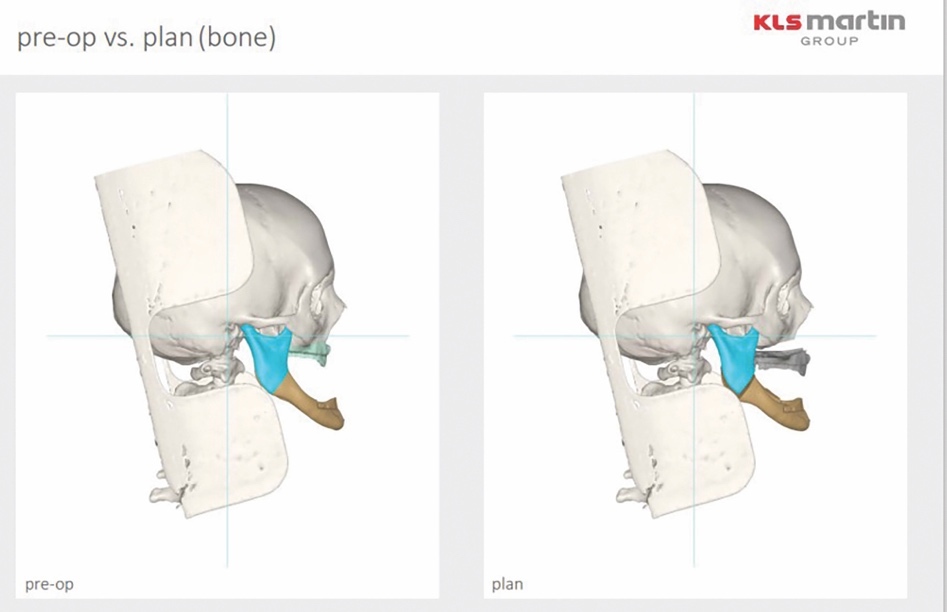
The use of a virtual 3D computer-aided planning system (KLS Martin) allowed the clinicians to accurately plan orthognathic surgical movements and acted as an excellent communication tool when communicating with the patient (Figure 11).
_outlining_pre-_and_postoperative_orthognat.jpeg)
Restorative management
In 2013, the patient had been deemed unsuitable for standard Straumann implants due to insufficient bone. Polyetheretherketone (PEEK) implants were also unsuitable as there had not been a healing technology assessment of their efficacy in relation to this particular clinical situation, and further research and clinical trials are still required to explore the application of this material in orthognathic surgery.23
Careful digital restorative planning enabled a functional and aesthetically pleasing outcome to be achieved with a maxillary bridge and a mandibular implant-retained and -supported denture (Figures 12 and 13). Enhancements in the speed of osseo-integration, the strength of dental implants and the range of prosthodontic materials contributed to the restorative success.


Multidisciplinary team planning
MDT planning was central to the success of the case, integrating input from OMFS, restorative dentistry and orthodontics, with careful surgical sequencing and patient-specific considerations. As noted in the aforementioned meta-analysis,17 piezoelectric techniques offer enhanced safety and control, particularly in delicate anatomical areas, further justifying their benefit in this case. While the use of the piezoelectric saw was technically significant, it was the MDT’s collaborative decision-making that led to this choice and ensured optimal patient safety and outcomes.
Conclusions
Treatment in this case has involved a lengthy course of OMFS and restorative treatment, including multiple MDT clinics. The two-stage surgical approach, with careful planning by OMFS, restorative dentistry and orthodontics, allowed for adequate bony healing and the successful placement of dental implants in a patient with ED, hypodontia and a hypoplastic maxilla. This interdisciplinary care was crucial in achieving a successful outcome for this patient. This case also demonstrates the favourable use of piezoelectric saws in the osteotomy of an underdeveloped maxilla. All patients with ED, and with concerns regarding their skeletal profile or dental function, should be referred onwards by their general dental practitioner for MDT planning. This will allow for all available treatment options to be discussed and for the patient to make the best-informed decision on their treatment.
Ethical statement
We can confirm that written informed consent for publication was obtained from the patient who was included in this case report.