Introduction
Incidence of oral cancer
Oral cancer is ranked as the 13th most common cancer worldwide with an estimated 377,713 new cases and 177,757 deaths in 2020.1 Tobacco, alcohol and betel quid use, and the presence of an oral potentially malignant disorder (OPMD), e.g., oral leukoplakia, are recognised as the main risk factors for oral cancer,1 with up to 80% of oral cancers occurring in smokers.2 While the synergistic effect of tobacco and alcohol is well documented,2 other risk factors such as being male, older age, South Asian race, low socioeconomic status, and low consumption of fruit and vegetables are also associated with an increased risk of oral cancer.3 Research has shown that public awareness of oral cancer ranges from 56% to 72%,4–6 and in particular there are varying levels of awareness of the associations between gender and age and oral cancer. Lack of awareness of the signs and symptoms of oral cancer can lead to misattribution, and this has been reported as the most common reason for a delay in seeking help for the common signs and symptoms.7,8
As the early stages of oral cancer development are often asymptomatic, screening provides an opportunity for early detection of both oral cancer and OPMDs.9 Signs of early oral cancer can be identified by trained healthcare professionals with limited special equipment10 and even by individuals themselves if sufficient education is provided.11 Despite the ease of detection of oral cancer, approximately one-third of patients wait more than three months before consulting a healthcare professional about signs of oral cancer.8 Existing research suggests that opportunistic screening of high-risk individuals is valuable in early cancer detection and down-staging of the disease,9,10 resulting in more favourable long-term outcomes for the patient.7
Unfortunately, the incidence and mortality rates of mouth and pharyngeal cancer in the Irish population have been gradually increasing for the past 25 years, with oral cancer accounting for 44% of these cases (ICD CO2-CO6).12 The highest incidence of this cancer is recorded in males, where it is most commonly seen in 60-66 year olds. In females it is most prevalent in 50-64 year olds.12 The overall five-year survival rate still remains poor despite advances in treatment (53%), with early stage at diagnosis being the most important factor in improving prognosis.12 Therefore, it is pertinent to investigate the awareness of oral cancer in an Irish cohort.
The purposes of this study were to: i) assess the awareness of the signs and symptoms of oral cancer and its risk factors in an Irish patient cohort; and, ii) examine the awareness and attitudes of this patient cohort towards oral cancer screening.
Methods and materials
Study design
This was a cross-sectional pilot study. Ethical approval was obtained from the Research Ethics Committee, School of Dental Science, Trinity College Dublin (approval number DSREC02022-02). This study is reported using the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) cross-sectional reporting guidelines.13
Setting
Patients waiting for appointments for various dental clinics through routine, emergency and referral pathways were approached in the waiting area of the Dublin Dental University Hospital (DDUH) lobby by one of the investigators between August and October 2022, and invited to participate in the study. All consecutive attendees were supplied with a participant information leaflet (PIL) and consent form, and details of the study were discussed. Versions of the consent form and questionnaire were available both on paper and online via a QR code link to SurveyMonkey.
Participants
Inclusion criteria were patients over the age of 18, with no prior history of cancer other than non-melanoma skin cancer, attending dental clinics in the DDUH. Patients attending the oral mucosal dysplasia clinic and post-oral cancer treatment clinics were excluded from participation.
Data collection
Participants were asked to self-complete the previously validated questionnaire9,14 containing 32 questions on socio-geographic parameters, lifestyle factors, and validated items examining participants’ beliefs, awareness, knowledge and experience of early detection of oral cancer and its risk factors.14–17 The questionnaire took approximately 10 minutes to complete. All data were anonymised and no personal details were identifiable.
Statistical analyses
Power analysis calculation for this study was not performed, as this was a pilot study in an Irish cohort. Descriptive analyses were used to describe the characteristics of the participants. The data were analysed using RStudio (Version 4.2.2). Pearson’s Chi-squared, Fisher’s exact, and Fisher’s exact with simulated p values based on 2,000 replicates, tests were used as appropriate, and a table of counts and percentages generated. Logistic regression, to determine odds ratios and confidence intervals (CI), was carried out using the R packages epiR and car, and multinomial regression was carried out using the R package nnet.
Results
Participants
A total of 124 individuals were recruited, and 10 other individuals declined to participate. One respondent was excluded from the analysis due to a history of melanoma. Only two participants completed the online version of the questionnaire, while the remainder completed the paper version.
Sociodemographic parameters
The mean reported age of the participants was 45 years (range 18-89). Age was categorised into groups of 18-39 (32.4%), 40-60 (51%), and over 60 years (16.6%), for analysis.
Risk factors
Audit-C scores were calculated and revealed that almost one-third of the respondents (31.1%) had scores indicating severe and high-risk alcohol use. One-quarter (24.4%) were current smokers, with the majority of these (67.7%) smoking 10 or more cigarettes per day. A total of 42 respondents indicated that they were former smokers, with 54.8% of these having stopped smoking more than 10 years previously. There were no statistically significant associations in relation to lifestyle factors.
In relation to previous dental visits, 65.6% of participants reported that they had visited a dentist in the past year, 10.7% had visited within the past one to two years, and 23.8% had not visited for at least two years. Some 39% of respondents visited their dentist for a regular check-up at least annually, 17.2% visited less regularly for an occasional check-up, and 43.4% only visited when having trouble with their teeth.
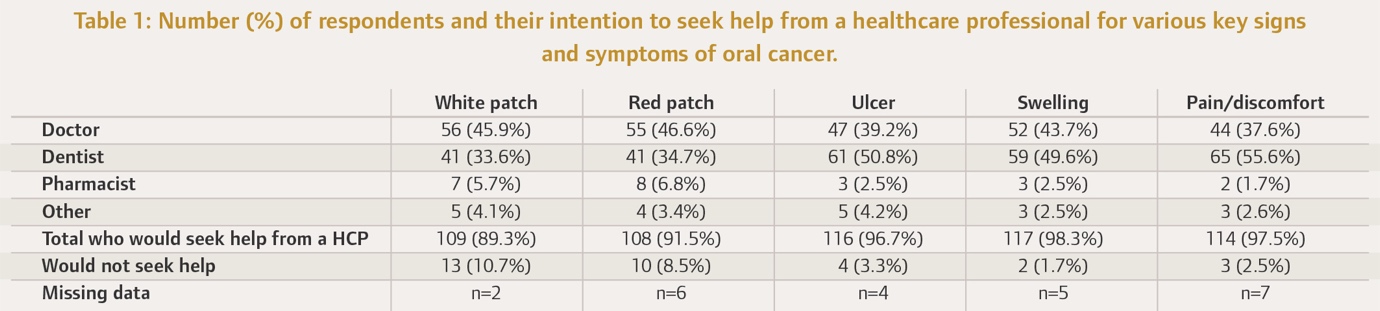
Participants were asked if they would seek help for various key signs and symptoms of oral cancer and, if so, which healthcare professional (general medical practitioner (GMP), dentist, pharmacist, or other) they would attend. Nearly half of the respondents reported that they would seek help from their GMP for an oral white patch (45.9%) or red patch (46.6%), while only 33.6% and 34.7%, respectively, would attend their dentist for these lesions. On the other hand, the participants were more likely to seek help from their dentist than their GMP for an oral ulcer, oral pain/discomfort, or an oral swelling (Table 1).
_of_respondents_and_their_intention_to_seek_help_from_a_healthcare_professional_f.jpeg)
Oral cancer awareness and knowledge
Although 69.7% of respondents had heard about oral cancer, the majority of these (83.7%) indicated that they knew nothing or very little about it. With regard to knowledge of risk factors for oral cancer, the majority could not identify the use of betel nut (90.5%) or male gender (80.2%) as risk factors. Surprisingly, 35.3% failed to recognise alcohol consumption, 22.5% chewing tobacco, and 12.8% smoking, as risk factors.
Interestingly, males were 4.88 times more likely to know that male gender was associated with an increased risk of oral cancer (adj OR 4.88, padj=0.02) than females. No statistically significant associations between gender, age, educational level, and awareness of the signs and symptoms of oral cancer and its risk factors were found.
Oral cancer screening awareness and attitude
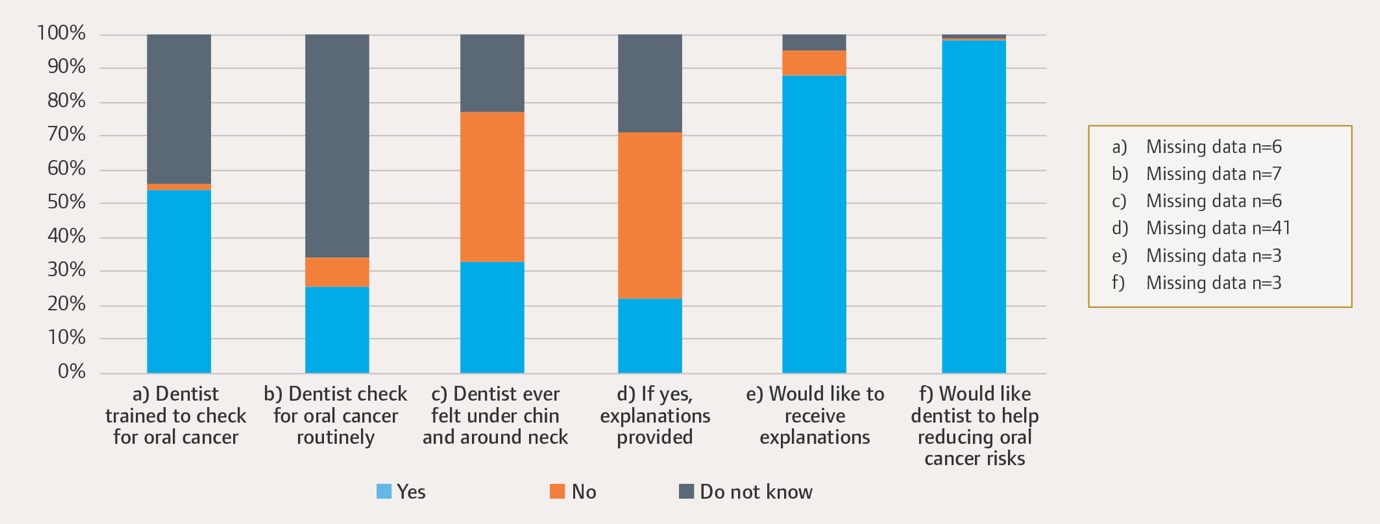
Figure 1 summarises participants’ awareness of oral cancer screening. Almost half of the respondents (45.8%) did not know that dentists were trained to identify signs and symptoms of oral cancer and only one-quarter (25.6%) were aware of being routinely checked for oral cancer at their dental visits. Those aged 40-60 years were 4.74 times more likely to know that dentists were trained in oral cancer screening (95% CI 1.84-12.15) than those aged 18-39. Almost all respondents (87.6%) would like their dentist to tell them if they were checking for signs of oral cancer and 98% would like their help in reducing their risk of developing it.
Overall, most respondents (98.3%) had a positive attitude towards having an oral cancer screening.

Discussion
This cross-sectional study was designed to assess awareness of the signs and symptoms of oral cancer and its risk factors, as well as experiences and attitudes towards oral cancer screening, in an Irish patient cohort. It should be noted that the results present the views of a convenience sample of patients from one institution and so sampling bias cannot be excluded.
Knowledge of oral cancer was poor, with less than one-fifth of respondents (16.3%) indicating some knowledge. This figure is similar to reports from studies in the UK (19%)5 and Australia (25%),18 but shows some improvement from an earlier study in Ireland (6%).11 However, the majority of respondents understood that smoking (87.2%) and alcohol consumption (64.7%) were risk factors for oral cancer, similar to a study in Portugal,6 where 89.5% of individuals identified tobacco, and 63% alcohol, as causes of oral cancer. Knowledge in relation to alcohol was higher than demonstrated in earlier UK and Ireland reports, where only one-fifth and one-tenth of respondents identified it as a risk factor for oral cancer,4,11,19 suggesting an improvement in public awareness of the risks of alcohol consumption. However, knowledge of other risk factors was poor, including male gender (19.8%) and betel quid use (9.5%). These were consistent with results from other studies, where only 22% of respondents identified male gender6 and 12% betel quid use20 as risk factors. The low knowledge on chewing betel quid is unsurprising, as 84.4% of our cohort was Caucasian, with only 6.8% being Asian/Asian Irish. It is interesting to note that men in our study were significantly more likely than women to know that male gender places them at increased risk for oral cancer. The basis for this increased knowledge among men is not clear; however, it may be part of a general awareness among men that they are more likely to be diagnosed with a cancer in their lifetime than women. While the results in relation to tobacco and alcohol awareness are encouraging, there is still a clear need to educate the general public with regard to these and other common risk factors for oral cancer. Similarly, it is important to educate patients about clinical presentations of oral cancer and the display of diagnostic toolkits in waiting rooms is a simple possible measure.
Exploiting every opportunity for oral cancer screening is vital for early cancer detection and hence, improved survival. Unfortunately, only 15% of mouth and pharyngeal cancers presented at stage I, while 49% presented at stage IV, in the 2014-2018 interval.21 The sample demonstrated a positive attitude towards oral cancer screening (98.3%), with most professing that they would not be particularly anxious about having this carried out (80.2%). Only one-quarter were aware of being routinely checked for oral cancer at their dental visits, which was consistent with other studies (14-47%).5,20,22 This indicates a need for clear communication from dentists that a routine check-up appointment entails not only a dental review but also examination of the oral mucosa for signs of oral cancer and other oral mucosal diseases.
It is reassuring that the majority of the respondents would consult a healthcare professional for each of the signs and symptoms of oral cancer. This study identified that patients preferred to visit their doctor instead of their dentist in relation to an oral white or red patch. There was a small percentage of respondents who would seek help in relation to signs and symptoms of oral cancer from other healthcare professionals, such as pharmacists. While dentists are trained to examine soft tissues and detect oral cancer, there is varying knowledge among healthcare professional groups when it comes to recognition of signs and symptoms of oral cancer. One Irish study explored knowledge among non-consultant hospital doctors and reported that only 19% of respondents regularly examined the oral mucosa during consultations, with many exhibiting a lack of knowledge of how to diagnose oral cancer based on clinical appearance.23 Rogers et al. reported that 82% of pharmacists could identify a non-healing ulcer but fewer identified white (52%) and red (57%) patches as possible oral cancer.7
Irregular dental attendance is associated with an increased risk of head and neck cancer22 and it is a significant cause for concern that nearly a quarter of respondents had not attended a dentist in the previous two years. Funding of the public dental service has fallen dramatically in both Ireland and the UK in the last 10 years, leaving more people without access to regular dental care.24,25 This makes it increasingly likely that patients will seek the advice of other healthcare professionals in relation to oral signs and symptoms. Therefore, the wider healthcare team should be trained to recognise oral cancer signs and symptoms, and to refer in a timely manner.
The study did not find any statistically significant relationship between gender, age, and educational level, and either awareness of the signs and symptoms of oral cancer and its risk factors, or with experiences and attitudes towards oral cancer screening. These results differ from previous studies, which indicated that female gender and high occupational and educational status were associated with increased awareness of oral cancer and its risk factors.5,19,22 Our results indicate that the age group 18-39 years were the least aware of the availability of oral cancer screening from their dentists. This is not surprising, as it has been recently reported in the UK20 that general awareness of oral cancer usually increases with age. Therefore, education of younger age groups is needed for improving oral cancer awareness in the general population, particularly in view of the increasing incidence of the disease.
Strengths
This study was the first to assess awareness of the signs and symptoms of oral cancer, its risk factors, and experiences and attitudes towards oral cancer screening in an Irish cohort. Previously, a study of people attending Mouth Cancer Awareness Day was completed by MacCarthy et al., but mainly assessed attendees’ knowledge on self-examination and dental attendance, with a small number of questions relating to habits or activities that might cause oral cancer.11 Contrary to our study, where individuals attended for routine dental care, the attendees in the MacCarthy et al. study were attending as part of an oral cancer awareness campaign and could be considered more informed than the current study population.11 Our study is adding new information on association analyses between gender, age, educational level, and either awareness of the signs and symptoms of oral cancer and its risk factors, or with experiences and attitudes towards oral cancer screening.
Limitations
We acknowledge that we surveyed a convenience sample attending a dental hospital’s outpatient clinics for a range of dental procedures, and this may have introduced some bias. Therefore, the results may not be representative of the general Irish population.
Recommendations
-
Collaboration with the wider team of healthcare professionals in non-dental settings on public awareness of oral cancer and the importance of opportunistic screening is desirable.
-
Oral cancer public awareness campaigns, targeting all age groups, based on tested interventions, should be developed.
-
The dental team should avail of every opportunity to educate patients about the risk factors for oral cancer, and inform patients that an oral mucosal screening for oral cancer forms part of their routine dental reviews.
Conclusion
This pilot study indicates a lack of knowledge of some of the risk factors, signs and symptoms of oral cancer in our study population. It also demonstrated a lack of public awareness of the role of dentists in screening for oral cancer. This study should be repeated in a larger cohort in non-dental settings. The information obtained will be useful in designing and implementing oral cancer awareness programmes and initiatives, which should particularly target those areas where awareness is lacking.
Acknowledgements
We would like to thank all participants for completing the survey. We would also like to thank Adam McQuillan for helping with data entry.