
Introduction
Interproximal reduction (IPR) involves mechanical reduction of the mesiodistal dimensions of teeth.1,2 This procedure can be used to create space for relief of crowding, address tooth size discrepancies (TSDs), reduce black triangles, and promote stability of the lower labial segment.3–7 IPR is frequently used in combination with clear aligner treatment, but may also be used in conjunction with treatment involving other appliances, such as fixed, functional or retention appliances.8 Recent surveys have indicated a trend for increased use of IPR by both general and specialist practitioners in conjunction with aligner treatment and a decline in tooth extraction for the relief of crowding.9–11
Questionnaire surveys in North America and India have explored use and perceptions of IPR by dental professionals.12–14 IPR was used most frequently to address TSDs, relieve anterior crowding, improve aesthetics, create space in borderline extraction cases, and to reduce relapse. Handheld strips were mostly employed and postoperative fluoride treatments were infrequently prescribed.14 The concern expressed by clinicians in regard to caries development and postoperative sensitivity following IPR differed between surveys.12–14 Respondents to North American surveys felt that IPR posed little caries risk (95%)14 and seldom applied topical fluoride postoperatively (40%12 and 27%14), while a sample of orthodontists in India felt that teeth were more susceptible to caries (91%) and sensitivity (55%) after IPR, applying topical fluoride frequently (87%) to reduce these risks.13
With the use of IPR on the rise,11 it is timely to further explore this procedure. To date, there is no evidence available on how IPR is used by orthodontists in the Republic of Ireland (RoI), or their perceptions of this procedure. The aim of this study, therefore, was to ascertain orthodontist-reported practices and perceptions regarding IPR.
Materials and methods
Ethical approval was granted by the Clinical Research Ethics Committee of the Cork Teaching Hospitals. Postal and electronic versions of a de novo questionnaire were developed for orthodontists with reference to previous surveys.8–10,12–14 The questionnaire was formulated and pre-piloted internally according to recommended guidelines, and modified following feedback on the order of questions and formatting.15,16
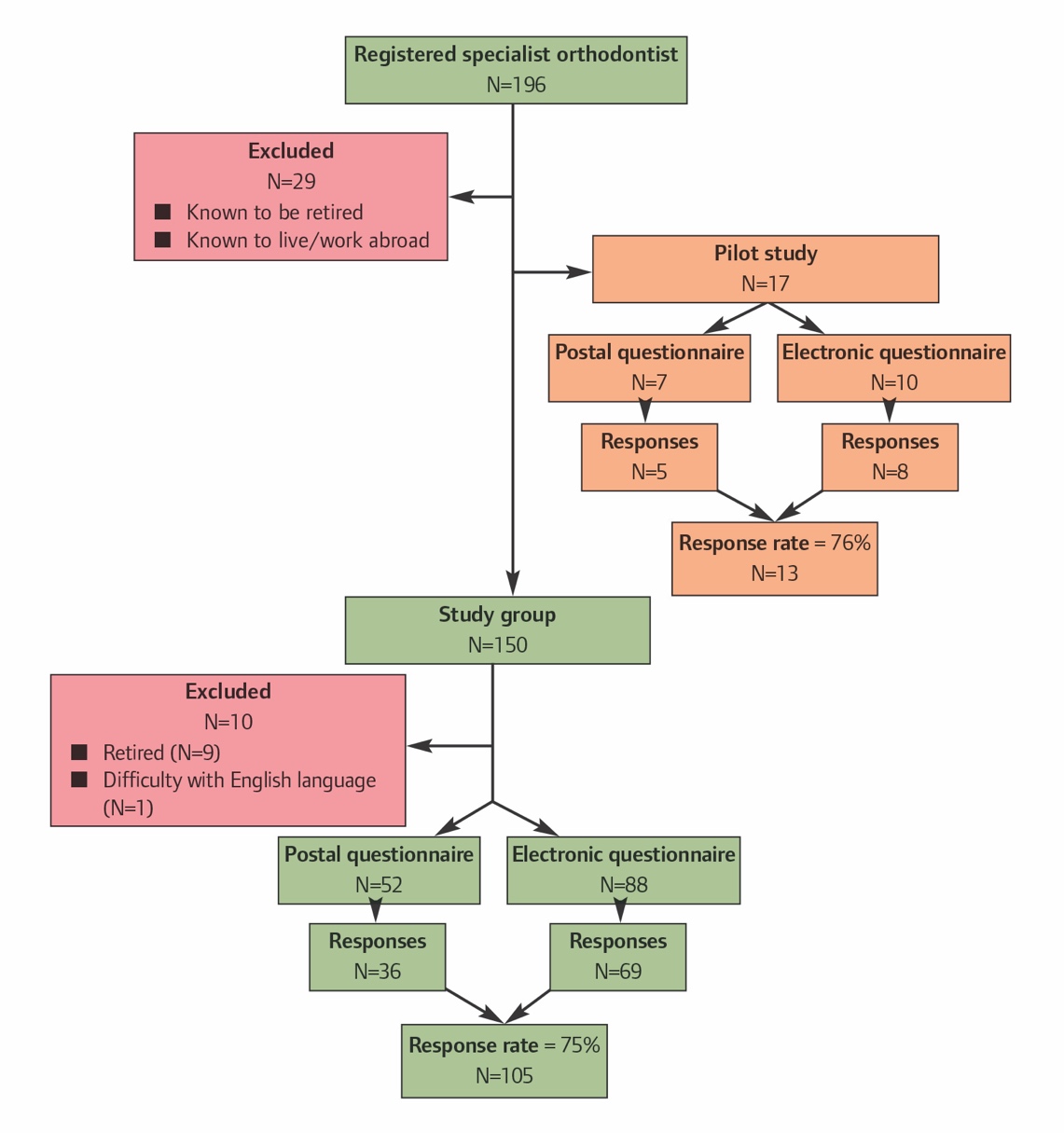
The Dental Council of Ireland’s Specialist Register, Division of Orthodontics, and the Orthodontic Society of Ireland’s membership list were used to generate a database of participants. Using a random sequence generator (www.random.org/sequences), the survey was initially piloted with 17 orthodontists, approximately 10% of the total sample. All were contacted by telephone by one author, provided with an overview of the study, and invited to participate. Following consent, the option of receiving a postal or electronic version of the questionnaire was offered. Those uncontactable by telephone after three attempts were sent the postal version of the questionnaire by default. Those who lived abroad or had ceased to practise were excluded. All responses were anonymised. After one month, non-responders were sent one reminder to complete the survey. Responses to this pilot survey were not included in data analyses.
After piloting, minor modifications to question coding and survey layout were made prior to distribution. The final sample (n=140) was then surveyed using the same methodology as the pilot group. Results were analysed descriptively.
Results
Demographic details
Responses were received from 105 orthodontists (75% response) (Figure 1), comprised of 57 males and 48 females. The average time in practice was 15.5 years (range 1-45 years). Most trained in the UK (53%), followed by the RoI (27%). The remainder trained in the US (7%) and other countries (13%) including Bulgaria, Canada, Greece, Hong Kong, Hungary, Poland and Romania. The majority worked in private practice (59%), followed by State-funded practice (21%) or a mixture of private and State-funded (11%), with the remainder a mix of private practice, State-funded and teaching hospital (6%), private practice and teaching hospital (2%), and teaching hospital only (2%). Most (77%) received IPR instruction during postgraduate training using strips, handheld (63%) or in a holder (50%).

IPR practices: indications and uses
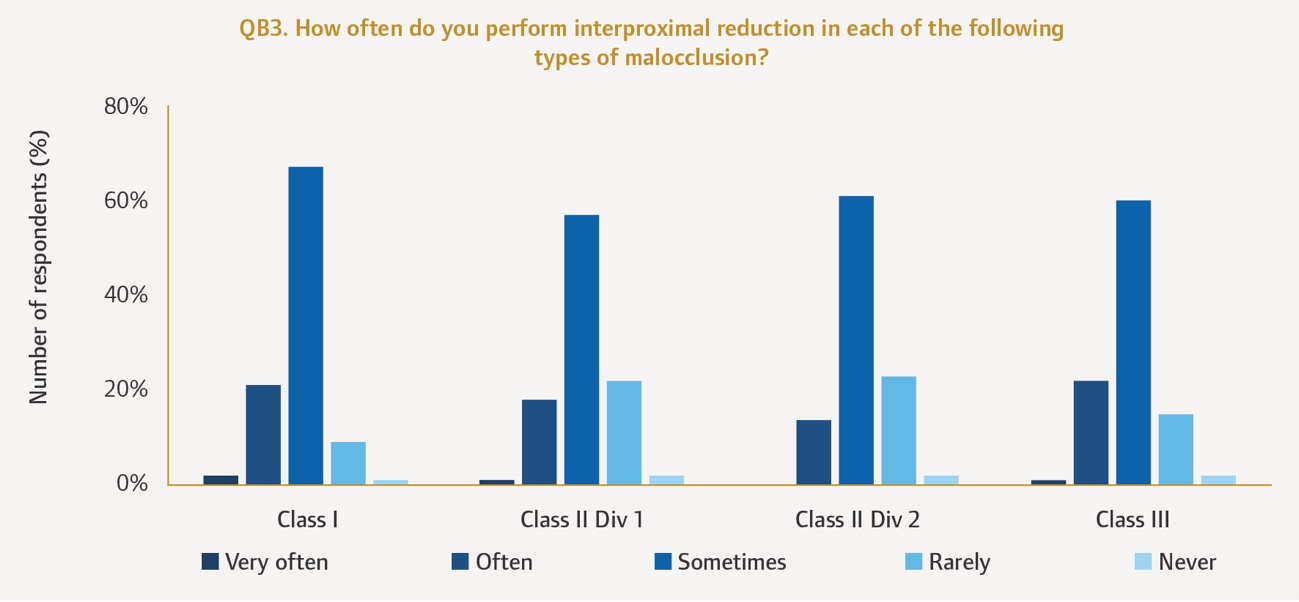
Nearly all (98%) orthodontists reported that they performed IPR, and almost half (47%) of orthodontists used IPR routinely. More orthodontists reported increasing (44%) than decreasing (6%) frequency of IPR use over the past five years, while 50% reported no change. IPR was most often used in adults, followed by adolescents in the permanent dentition. Little difference existed in frequency of use of IPR across malocclusions (Figure 2). IPR was undertaken primarily after initial alignment and least commonly during retention (Figure 3). Use was most frequent with aligner treatment (59%) or fixed appliance treatment (33%) and least with functional appliances (1%). IPR use did not influence retainer choice for most respondents (92%). IPR was used for triangular-shaped teeth (97%), reshaping existing restorations (92%), addressing TSDs (89%), and reducing black triangles (66%). Mild crowding was considered an indication for IPR (92%), and less so for moderate (40%) or severe (12%) crowding.
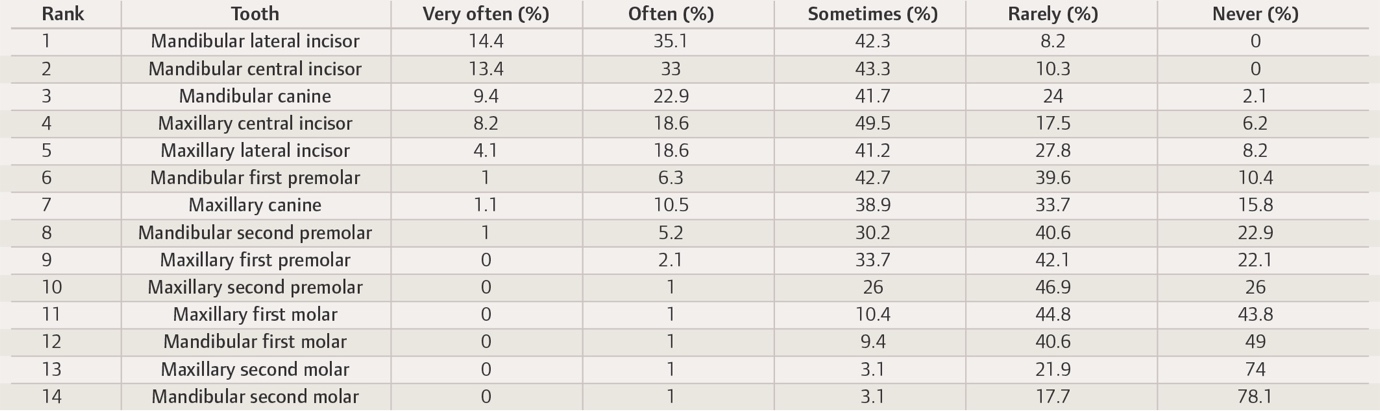
Mandibular anterior teeth in the order of lateral incisors, central incisors, and canines were most frequently reduced, followed by maxillary central and lateral incisors. IPR was less frequently used posteriorly in the mouth (Table 1).



IPR practices: procedure
Prior to IPR, only 26% undertook a Bolton analysis (which is used to assess if there is a tooth size discrepancy by comparing the sizes of maxillary and mandibular teeth).17 A preference was indicated for 0.3mm enamel removal from proximal surfaces of upper (43%) and lower anterior teeth (38%), and 0.4mm for posterior teeth. Most (60%) opted for space creation of 2-4mm maximally per arch with IPR.
The majority (82%) performed IPR over several visits, with handheld strips (87%), strips in holders (58%), or with diamond burs in an air rotor (51%). Almost half (47%) measured tooth reduction with a leaf gauge. Most (93%) recorded the teeth reduced but fewer (64%) recorded the amount of enamel reduction per tooth. After IPR, the use of fluoride mouthwash (57%) and interdental brushes (51%) was encouraged, but recontouring (44%), polishing (45%), or treatment of enamel surfaces with fluoride (24%) or amorphous calcium phosphate products (6%) was undertaken less frequently.
Written information on IPR for patients was provided by a minority (11%). Of those who did, most gave the information leaflet developed by the British Orthodontic Society (BOS).18 Risks of pain (71%), sensitivity (34%), gingivitis (15%), and caries (12%) were routinely discussed with patients, as were benefits such as reducing black triangles (94%), relief of crowding (94%), improvement in tooth shape (93%) and size (83%), avoidance of extractions (72%), and improved stability (49%).
Perceptions of IPR
IPR was perceived to be easier to perform anteriorly than posteriorly (87%). Orthodontists felt that IPR posed little caries risk to patients (72%). Some 62% had researched the effects of IPR and indicated a willingness to have IPR carried out on themselves (87%). Orthodontists perceived their patients to find IPR uncomfortable (48%) rather than painful (9%), and preferable to extraction (71%).
Orthodontists perceived their patients’ level of pain during IPR to be 3.3/10 (range 0-7) and a minority (2%) reported that they had encountered postoperative sensitivity in their patients. Although considered easy for patients to understand (89%), few orthodontists (12%) reported that their patients were aware of IPR.
Discussion
While clinical considerations and short- and long-term effects of IPR have been studied,1,19 no previous survey has investigated the use and perceptions of IPR in contemporary orthodontic practice in the RoI. The 75% response achieved in this survey is considered ‘extremely good’,15 and higher than the response to similar surveys, which ranged from 0.92-66%.8,10,11
Reported use of IPR by 98% of orthodontists was in keeping with previous studies where 89-100% use was described.12–14 Some 44% of respondents indicated increased use over the past five years, which supports the trend observed in UK and Belgian surveys.10,11 Data gleaned from 2014 and 2020 North American studies revealed no change in the frequency of IPR use but a very low response (0.92%) precluded meaningful conclusions.8 The instruments used, indications for use, and the conservative amount of enamel reduction reported in the present study align with previous findings.8,12 Postoperative enamel recontouring, polishing or surface treatment with fluoride or other agents were not routine, suggesting a perception among orthodontists that IPR poses a minimal iatrogenic risk, in agreement with existing literature.1,19
Almost two-thirds of respondents indicated that they had researched the effects of IPR on dental health, fewer than had done so in North America (81%).14 Orthodontists in both surveys were amenable to having IPR performed on themselves (87% and 92%, respectively).14
As orthodontists perceived their patients to be unfamiliar with IPR before the procedure, this highlights that further information may be needed to assist with informed decision-making.20 Patients were also perceived to find IPR uncomfortable rather than painful, and preferable to extraction.
The strengths of the present study include its high response and specific focus on IPR, which heretofore has received limited coverage in surveys. Responses were restricted to orthodontists who were registered and working in one country, but the wide range of locations where orthodontists were trained limits this impact. In addition, this survey provides new baseline data on the practice of IPR in the RoI, to which comparison can be made by other researchers. With all surveys, practices and perceptions were self-reported, which may differ from actual practice.
Future research could investigate IPR use among general dental practitioners who practise orthodontics, especially considering the widespread adoption of IPR with clear aligner treatment.
Conclusions
Conservative IPR of less than 4mm per arch was mostly undertaken for teeth in the lower labial segment, in adults or adolescents, in conjunction with aligner or fixed appliance treatments. Handheld strips were most commonly used. Orthodontists perceived their patients to be unfamiliar with IPR, and to find it uncomfortable rather than painful, and preferable to extraction.